At a Glance
• Scleral buckling has been a successful technique used to repair rhegmatogenous retinal detachment since it was first introduced in the 1950s and is the preferred treatment modality for many indications.
• The use of a chandelier endoillumination system improves visualization and treatment of retinal breaks during scleral buckling surgery and may restore favor for the technique.
• Chandelier-assisted buckling may also limit or completely eliminate the need for indirect ophthalmoscopy, which in turn may lessen the prevalence of related musculoskeletal injuries among retina specialists.
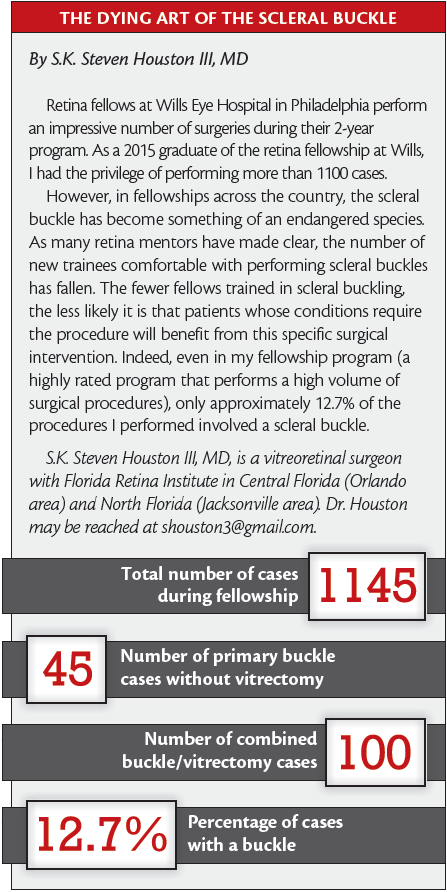
Since its introduction in the 1950s,1,2 scleral buckling has been a highly successful technique for the repair of rhegmatogenous retinal detachment. However, the popularity of this time-proven treatment appears to be waning (see “The Dying Art of the Scleral Buckle").3
The decreased practice of scleral buckling may be due in part to recent advances in the machines, instrumentation, and visualization systems for pars plana vitrectomy (PPV), making PPV a more attractive procedure for vitreoretinal specialists. In addition, the inability of learners to observe their mentors employing intraoperative indirect ophthalmoscopy in scleral buckling poses an additional challenge that may limit its transfer to the next generation of retina fellows.
Despite these issues, scleral buckling is the preferred treatment modality for many indications. This surgical approach entails lower costs than PPV and avoids many of the potential complications and postoperative requirements associated with PPV.4,5 Scleral buckling also preserves the vitreous, which can be beneficial in the event that intravitreal injections, now commonly used to treat numerous retinal diseases, are needed in the future.
CHANDELIER-ASSISTED SCLERAL BUCKLE
The recent introduction of chandelier endoillumination during scleral buckling capitalizes on advances in visualization technology afforded by widefield intraoperative viewing systems through the operating microscope. This addition may be pivotal in reversing the trend of diminishing surgical preference for scleral buckling.
Aras et al described the first transscleral fiberoptic-assisted scleral buckle, which consisted of a conventional scleral buckling surgery performed along with visualization and treatment of retinal breaks under an operating microscope using a torpedo-style light source inserted through a noncannulated sclerotomy.6 Nam et al introduced the more commonly used technique, in which a small-gauge fiberoptic chandelier light source is inserted through a standard transscleral cannula.7 Since then, promising but limited data from around the world regarding the use of this technique and patient outcomes have been published.8-11
THE TECHNIQUE
Our preferred method of chandelier-assisted scleral buckling surgery begins with a conventional 360° conjunctival peritomy followed by isolation and looping of the rectus muscles. At every step of the procedure, visualization is done through the microscope instead of by indirect ophthalmoscopy.
A transscleral cannula is placed to house the chandelier fiberoptic illumination system. Upon insertion of the chandelier light source, we use the operating microscope with either a widefield contact lens or a noncontact wide-angle visualization system for scleral-depressed examination and treatment of retinal breaks by cryotherapy.
The primary retinal break is marked to determine the location for buckle placement, at which point the chandelier light is removed and the cannula is plugged. This allows easier placement of the buckle around the globe without hindrance by the chandelier light source. The buckle is then sutured in place without the need of the microscope, except in highly myopic patients or those with very thin sclera for whom suturing under the microscope may be safer.
After pulling on the buckle, the chandelier is reintroduced through the cannula for visualization of pulsations at the disc, performance of additional cryotherapy, and assessment of the relation of the retinal breaks to the supporting buckle. Drainage is also done under direct visualization when needed. Microscope-integrated optical coherence tomography can be used at this step to visualize the needle in the subretinal space for safer drainage.
ADVANTAGES OF THE CHANDELIER
The use of a chandelier endoillumination system improves visualization and treatment of retinal breaks during scleral buckling surgery. The combination of a wide-angle viewing lens with diffuse endoillumination provides excellent visualization of retinal breaks, even in the far periphery, ensuring accurate identification and precise cryotherapy of all breaks. Missed breaks are common causes of recurrent detachment for less experienced surgeons and trainees. This technique ensures treatment of all breaks while avoiding excessive or more posterior treatment.
This approach also improves teaching of the procedure. By permitting the use of the operating microscope and live video feed, this technique enables the demonstration of cryopexy for trainees and allows direct observation and guidance of treatment performed by trainees.
In addition, the ability for all surgical team members to simultaneously view all aspects of the operation appears to improve communication among the team members. This enhances efficiency, precluding the need to continually switch the indirect ophthalmoscope between faculty and trainees. This, combined with the benefit of better overall visualization through the cornea, potentially shortens the duration of the procedure.
Finally, by limiting or completely obviating the need for indirect ophthalmoscopy, the use of chandelier-assisted scleral buckling may help to reduce related musculoskeletal injuries, which are prevalent among retina specialists.12 In our experience to date at Duke University Eye Center, the use of a chandelier light source has not been associated with increased surgical time, iatrogenic retinal breaks, or other complications.
ADDITIONAL SURGICAL PEARLS
- We usually place our lighting system 180° away from the retinal breaks in pseudophakic patients for maximal illumination when indenting the light. However, we place the chandelier 90° away in phakic patients to avoid lens touch.
- Mild vitreous prolapse through the transscleral cannula is a unique risk of the chandelier scleral buckle, particularly when pulling up the buckle or injecting gas into the posterior chamber. To prevent this, it is necessary to plug the transscleral cannula when it is not occupied by the chandelier. We found the plug included with the Alcon 20-to-25-gauge adaptor satisfactory when using a 25-gauge Alcon nonvalved cannula. To further curtail the risk of vitreous extrusion, intraocular pressure can be reduced with creation of an anterior chamber paracentesis before removal of the chandelier light system. Be sure to cut any vitreous wick that presents through the cannula or after cannula removal with scissors.
- The sclerotomy site should be sutured after cannula removal.
CONCLUSION
Wide-angle visualization with chandelier endoillumination is a novel advancement that appears to bring a distinct advantage to the performance and teaching of scleral buckling. For appropriate patients, chandelier-assisted scleral buckling appears to provide several potential advantages over traditional buckling techniques. n

Tamer H. Mahmoud, MD, PhD, is a vitreoretinal surgeon at Duke University Eye Center in Durham, N.C. He states that he has no financial interest in the material discussed in this article. Dr. Mahmoud may be reached at tamer.mahmoud@dm.duke.edu.

Riikka E.K. Nomides, BS, is a medical student at Duke University School of Medicine in Durham, N.C. She states that she has no financial interest in the material discussed in this article. Ms. Nomides may be reached at reh31@dm.duke.edu.

Michael I. Seider, MD, is a vitreoretinal surgery fellow at Duke University Eye Center in Durham, N.C. He states that he has no financial interest in the material discussed in this article. Dr. Seider may be reached at michael.seider@dm.duke.edu.
1. Custodis E. Die Behandlung der Netzhautabloesung durch umschriebene Diathermiekoagulation und einer mittels Plombenaufnaehung erzeugten Eindellung der Sklera im Bereich des Risses. Klin Monatsbl Augenheilkd. 1956;129:476.
2. Schepens CL, Okamura ID, Brockhurst RJ. The scleral buckling procedures.V. Synthetic sutures and silicone implants. Arch Ophthalmol. 1960;64:868-881.
3. American Society of Retinal Specialists. 2012-2014 Preferences and Trends (PAT) Survey. www.asrs.org/pat-survey/pat-survey-archive [access for members only].
4. Figueroa MS, Corte MD, Sbordone S, et al. Scleral buckling technique without retinopexy for treatment of rhegmatogeneous: a pilot study. Retina. 2002;22(3):288-293.
5. Heimann H, Bartz-Schmidt KU, Bornfeld N, et al. Scleral buckling versus vitrectomy. Ophthalmology. 2008;115(9):1635; author reply.
6. Aras C, Ucar D, Koytak A, Yetik H. Scleral buckling with a non-contact wide-angle viewing system. Ophthalmologica. 2012;227(2):107-110.
7. Nam KY, Kim WJ, Jo YJ, Kim JY. Scleral buckling technique using a 25-gauge chandelier endoilluminator. Retina. 2013;33(4):880-882.
8. Yokoyama T, Kanbayashi K, Yamaguchi T. Scleral buckling procedure with chandelier illumination for pediatric rhegmatogenous retinal detachment. Clin Ophthalmol. 2015;9:169-173.
9. Kita M, Fujii Y, Kawagoe N, Hama S. Scleral buckling with a noncontact wide-angle viewing system in the management of retinal detachment with undetected retinal break: a case report. Clin Ophthalmol. 2013;3(7):587-589.
10. Nagpal M, Sidharth B, Navneet M. Scleral buckling for rhegmatogenous retinal detachment using vitrectomy-based visualization systems and chandelier illumination. Asia Pac J Ophthalmol (Phila). 2013;2(3):165-168.
11. Gogia V, Venkatesh P, Gupta S, et al. Endoilluminator-assisted scleral buckling: Our results. Indian J Ophthalmol. 2014;62(8):893-894.
12. Mehta S, Hubbard GB. Avoiding neck strain in vitreoretinal surgery: an ergonomic approach to indirect ophthalmoscopy and laser photocoagulation. Retina. 2013;33(2):439-441.



_1784132761.jpg?auto=compress,format&w=75)











