The Case for Phacovitrectomy

By Timothy G. Murray, MD, MBA
Patients with concomitant cataract and vitreoretinal pathology commonly have the two issues addressed in separate procedures, but there are several advantages to combining phacoemulsification and vitrectomy into one procedure (phacovitrectomy).
BENEFITS OF PHACOVITRECTOMY
Achieving two goals in one surgical event lowers the overall combined risk compared with performing two procedures. Combined surgery also accelerates the patient’s visual recovery.
The integration of advanced anterior and posterior segment technology into comprehensive phacovitrectomy devices has helped to facilitate performing combined surgery. With modern phacovitrectomy platforms, combined cases take less time, fluidics stability is far better than in the past, and corneal clarity is excellent. Small-incision phaco systems now allow the surgeon to maintain stability of the anterior chamber.
PROOF IN PRACTICE
We conducted a retrospective review of 142 patients with a variety of macular pathologies (epiretinal membrane, macular hole, vitreomacular traction, or complications of macular edema) and visually significant cataract undergoing microincisional vitrectomy surgery combined with phacoemulsification.1 Preoperative mean visual acuity was 20/80, and final mean visual acuity at 18 months was 20/32. That represents a significant improvement, with rapid, sustained visual rehabilitation.
Our current surgical approach is to use either 23- or 25-gauge microincisional vitrectomy surgery systems with a valved cannula. In these cases, we typically first place the trocars, then perform small-incision torsional phacoemulsification, which involves placing an in-the-bag IOL, followed by suturing the clear corneal wound. Using widefield viewing, we perform three-port pars plana vitrectomy. For fine macular work, we use a macular contact lens, indocyanine green staining to peel the internal limiting membrane, and intravitreal triamcinolone acetonide at the conclusion of the vitrectomy. With this technique, we have not had complications of hypotony, choroidal detachment, or endophthalmitis. In all cases, a posterior chamber IOL was placed, and in no case were we unable to manage the macular pathology.
IMPROVED INSTRUMENTS, IMPROVED OUTCOMES
For complex macular pathology, advances in surgical instrumentation have improved outcomes, limited patient concerns, and extended indications for microincisional vitrectomy surgery, which is now the evolving gold standard for the management of macular disease. Higher-speed cutting technology has improved the safety of procedures; for example, instances of unrecognized peripheral breaks during vitrectomy are now rare.
I use 23- or 25-gauge transconjunctival microincisional surgery for most cases of complex macular pathology. Modern vitrectomy systems provide highly stable fluidics control. The use of valved cannulas, enhanced illumination, and widefield imaging has improved surgical control and enabled excellent instrument access. In many cases, I now perform vitrectomy using the vitreous cutter probe without scissors or forceps. Doing so decreases surgery time and significantly improves postoperative visual recovery.
GREATER ADOPTION
It is likely that we will see a shift in the United States toward greater adoption of integrated approaches to anterior and posterior segment surgery in clinical practice as retina surgeons take advantage of the best technologies that become available. As always, our focus as vitreoretinal surgeons is to improve the quality of our patients’ vision while minimizing the risks of our procedures. The incorporation of combined phacovitrectomy seems ideally positioned to improve overall care for patients with concomitant macular pathology and cataract.
1. Villegas VM, Gold AS, Latiff A, et al. Phacovitrectomy. Dev Ophthalmol. 2014;54:102-107.
Timothy G. Murray, MD, MBA
• founding director of Murray Ocular Oncology and Retina; professor emeritus of ophthalmology and radiation oncology at Bascom Palmer Eye Institute, both in Miami, Fla.
• financial interest: consultant for Alcon
• tmurray@murraymd.com
![]()
A Japanese Perspective
By Yusuke Oshima, MD, PhD
More than three-quarters of vitrectomy surgeries in Japan are combined with cataract phacoemulsification surgery. In fact, in phakic patients 50 or older, combined phacovitrectomy is recommended over vitrectomy alone because it ensures safer, quicker surgery with no concern for intraoperative lens touch or postoperative cataract progression. Most vitreoretinal surgeons in Japan now use a 25-gauge transconjunctival microincision vitrectomy approach together with small-incision (2.75- to 2.2-mm) cataract surgery.
27-GAUGE PHACOVITRECTOMY
In my practice, we have pioneered the use of 27-gauge instrumentation for sutureless vitreoretinal surgery—currently the smallest instrument size manufactured for vitrectomy—in combination with cataract removal. This results in excellent wound architecture to successfully complete smaller self-sealing incisions and minimize any risk of wound leakage.
Surgeons who use a 23- or 25-gauge system for phacovitrectomy usually place the trocar cannulas for vitrectomy before starting cataract surgery because waiting to do so after cataract surgery may cause the iris to prolapse into the clear corneal wound. Those who use a 27-gauge system do not have to worry as much about this because the 0.4-mm wound size is small enough for smooth insertion and easy wound sealing after cannula removal at the end of surgery (Figure).
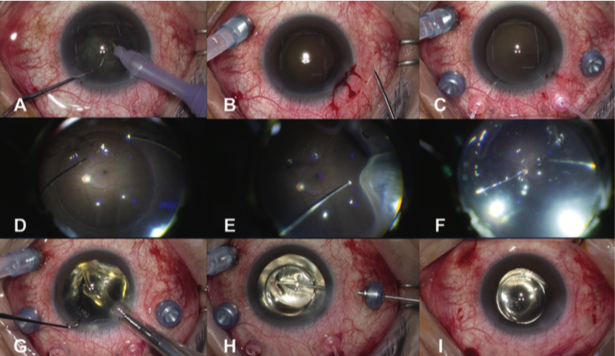
Figure. Phacoemulsification via 2.5-mm clear corneal incision (A). Angled insertion of a 27-gauge trocar cannula (B). Basic setting of the 27-gauge vitrectomy system for a primary retinal detachment case (C). Perfluorocarbon liquid injection via a 27-gauge blunt needle for flattening the detached retina (D). Peripheral vitreous shaving with a 27-gauge TDC cutter (E). Fluid-air exchange followed by endolaser photocoagulation (F). Acrylic IOL implantation through the clear corneal wound (G). Posterior capsulotomy using the 27-gauge TDC cutter (H). Conclusion of 27-gauge phacovitrectomy immediately after removal of all cannulas (I).
Using a single high-end machine to perform phacovitrectomy is convenient and saves space compared with use of two instruments. Our experience demonstrates good outcomes following combined microincisional cataract and vitreous surgery. I use two machines in my vitreoretinal and cataract practice: the Constellation (Alcon) and the VersaVIT 2.0 vitrectomy system (Synergetics). The Constellation operates at speeds of up to 7500 cpm for vitrectomy, and its dual pneumatic control cutter probe is an elegant solution for complex vitrectomy procedures. The VersaVIT 2.0 is a compact machine with functionalities similar to other single air pump venturi vitrectomy machines. A newly developed duty-cycle control cutter for use with the VersaVIT system also demonstrates nice vitreous cutting performance with top speed up to 6000 cpm.
In my practice, I recently connected an ultraspeed transformer (UST) from DORC to the VersaVIT 2.0 to enhance vitreous cutting speed. With the use of the twin duty cycle (TDC) vitrectome (DORC) with double cutting port, surgeons can achieve ultrahigh-speed cutting efficiency for faster vitrectomy because the double cutting port allows one to cut the vitreous twice with each stroke. Therefore, the TDC cutter with the UST, which gets its air pressure supply from the VersaVIT 2.0, theoretically has a cutting speed of up to 12 000 cpm. We tested the cutting efficiency of the 27-gauge double-port TDC vitrectome in our laboratory, and the results showed that cutting efficiency for vitreous removal was comparable to that achievable with conventional 25-gauge instrumentation.
Although tractional force may be a major concern with the design of the double cutting port, it can be minimized with the use of the 27-gauge TDC cutter. Even in the case of a primary retinal detachment, vitreous shaving can be done smoothly using the 27-gauge TDC cutter without any regard for tractional force.
CONSIDER COMBINING
Although minor complications may be encountered when phacoemulsification and vitrectomy procedures are combined, overall we have experienced no serious drawbacks. Phacovitrectomy eliminates the risk of cataract progression, the most common complication after vitrectomy, and that of posterior capsular opacification. The latter is avoided by cutting off the posterior capsule during the phacovitrectomy, which cannot be achieved when cataract surgery is performed after vitrectomy. Given these facts, phacovitrectomy also enhances permanent visual recovery. n
Yusuke Oshima, MD, PhD
• founder and director of Oshima Eye Clinic, in Takatsuki-City, Osaka; consultant at Nishikasai Inouye Eye Hospital, in Tokyo, Japan
• financial interest: consultant for Synergetics
• yusukeoshima@gmail.com




_1784132761.jpg?auto=compress,format&w=75)











