This year, two main areas will affect coding for retinal physicians: Current Procedural Terminology (CPT) and ICD-10-CM coding. This article addresses both and includes a selection of case studies that should be mastered as templates for this coming year.
CPT CHANGES
Descriptors Changed
The following codes have had their descriptors changed to read “including when performed” in lieu of “with or without.” Nothing has to be altered in your coding patterns; it is part of the CPT standardization of descriptors. The 2016 code descriptions (with changes in italics) are as follows:
67101 Repair of retinal detachment, one or more sessions; cryotherapy or diathermy, including drainage of subretinal fluid, when performed
67105 Repair of retinal detachment, one or more sessions; photocoagulation, including drainage of subretinal fluid, when performed
67107 Repair of retinal detachment; scleral buckling (such as lamellar scleral dissection, imbrication or encircling procedure), including when performed implant, cryotherapy, photocoagulation, and drainage of subretinal fluid
67108 Repair of retinal detachment; with vitrectomy, any method, including when performed air or gas tamponade, focal endolaser photocoagulation, cryotherapy, drainage of subretinal fluid, scleral buckling, and/or removal of lens by same technique
67113 Repair of complex retinal detachment (eg, proliferative vitreoretinopathy, stage C-1 or greater, diabetic traction retinal detachment, retinopathy of prematurity, retinal tear of greater than 90 degrees), with vitrectomy and membrane peeling, including when performed air, gas, or silicone oil tamponade, cryotherapy, endolaser photocoagulation, drainage of subretinal fluid, scleral buckling, and/or removal of lens
Descriptor Deletion of “1 or More Sessions”
Two CPT codes previously contained the phrase “1 or more sessions.” They now read as follows:
67227 Destruction of extensive or progressive retinopathy (eg, diabetic retinopathy), cryotherapy, diathermy
67228 Treatment of extensive or progressive retinopathy (eg, diabetic retinopathy), photocoagulation
The significance of this change is that the global period has been reduced from 90 days to 10 days, so that each treatment session may be billed as long as the procedure is performed outside of the global period. In actuality, the total global period is 11 days because the 10-day countdown begins the day after surgery.
The advent of the new the global period changes the classification of the procedure from major to minor. The Centers for Medicare and Medicaid Services regulations package payment of the office visit with that of the minor procedure. Caution is warranted when using modifier 25 to obtain payment for the office visit and should only be used if there is a separate and significant condition.1 This is rarely valid when performing repeat treatments and there would be no medical necessity for using the comprehensive eye code .
Code Deleted
67112 Repair of retinal detachment; by scleral buckling or vitrectomy, on patient having previous ipsilateral retinal detachment repair(s) using scleral buckling or vitrectomy techniques
CPT states, “67112 has been deleted. To report see 67107, 67108, 67110, 67113.” When performing a repeat retinal detachment repair on a patient who had prior surgery in the global period, code the procedure being performed and use the appropriate modifier (58, 78, or 79). If the surgery is not being performed in the global period, then no modifier is needed.1
Clarifications
The following now appears before all destruction codes
(ie, using such techniques as cryotherapy, diathermy, photocoagulation, and ocular photodynamic therapy): “Codes 67208, 67210, 67218, 67220, 67229 include treatment at one or more sessions that may occur at different encounters. These codes should be reported once during a defined treatment period.”
ICD-10-CM CODING MISHAPS
Although fewer problems than anticipated have emerged with ICD-10-CM, some have occurred. Many electronic health record (EHR) systems provide some degree of coding, but not necessarily the correct or pertinent code(s). The accuracy of the EHR is dependent upon the physician’s chart documentation provided in the record, particularly in the “Impression and Plan” areas. Following is a brief review of some issues that have arisen that may also require your attention.
• When listing your diagnoses for an encounter, start with the most serious. Claims are often paid based on the primary diagnosis, although others may be required. Thus, it is critical to put them in order of importance.
• Clinical problems for which a colleague is treating a patient should not be part of your office visit code diagnosis selection.
• With the organization and wording of ICD-10-CM, it may be difficult for your billing department to pick the correct code. Physicians who work with their staffs on these issues will have better claims processing results.
• For trauma/injury/complications of implanted material codes (T codes for Injury, Poisoning, and Certain Other Consequences of External Causes), it is important to add the A, D, or S and use the “x” placeholder when needed to ensure putting the A, D, or S in the 7th character position.
• The Local Coverage Determinations (LCDs) that Medicare Administrative Contractors (MACs) have issued may be missing ICD-10-CM diagnoses. Your claim will be denied if the diagnosis is not on the LCD list. The physician or staff member should notify the MAC of this problem; the MAC will be happy to fix it if it is legitimate. It is probably easier to work through your state’s ophthalmic society or a member of the MAC’s Carrier Advisory Committee.
CASE STUDIES
The following case studies combine the more difficult aspects of CPT and ICD-10-CM coding.

Case No. 1
History
Patient presented with retinal detachment and epiretinal membrane (ERM) in the right eye. Prior retinal detachment repair had been performed, but the surgery had not been performed in the global period. There also was silicone oil droplet coating of a previously inserted intraocular lens. Surgery consisted of (i) pars plana vitrectomy (PPV) repair of retinal detachment with endolaser; (ii) peeling of the ERM using indocyanine green (ICG) dye; (iii) removal of the dislocated IOL from the posterior segment; (iv) insertion of anterior chamber IOL; and (v) suture fixation of IOL under scleral flaps. Code all procedures.
Diagnosis Codes
- H33.001 Retinal detachment with retinal break, right eye
- H35.371 Puckering of macula, right eye
- T85.22xA Displacement of intraocular lens
- H27.01 Aphakia, right eye
- Z98.89 Personal history of surgery
Tips
Laterality determination (eg, right eye, left eye) has to be designated for each CPT code as well as the ICD-10-CM code. The fact that there is laterality designation on the ICD-10-CM code does not serve both sets of codes.
Case No. 2
History
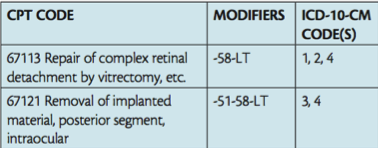
Patient presented with a retinal detachment, proliferative vitreoretinopathy, and ERM in the left eye. Prior retinal detachment repair had consisted of vitrectomy with endolaser photocoagulation, silicone oil, etc. Surgery performed in the global period consisted of (i) PPV repair of retinal detachment with endolaser photocoagulation; (ii) peeling of the ERM using ICG dye; and (iii) removal of silicone oil. Note that the first procedure had been coded 67108-LT (Repair of retinal detachment with vitrectomy…). Code all procedures.
Diagnosis Codes
- H33.42 Traction detachment of retina, left eye
- H35.372 Puckering of macula, left eye
- T85.698A Other mechanical complication of other
specified internal prosthetic devices, implants and grafts - Z98.89 Personal history of surgery
Tips
- Not all MACs require modifier 51.
- Modifier 58 is used with 67113 because it is a case of a more complicated procedure following a lesser procedure.
- Modifier 58 is used because the procedure is planned prospectively.

Case No. 3
History
Patient had sustained severe ocular trauma to his left eye and stated that broken glass had flown into the eye. Preoperative evaluation revealed a full thickness corneal laceration, traumatic cataract, posteriorly located retained intraocular foreign body, and vitreous hemorrhage. Surgery consisted of: (i) removal of glass foreign body located on the posterior aspect of the retina using forceps; (ii) PPV with endolaser and cryopexy; (iii) lensectomy for removal of traumatic cataract; (iv) repair of full thickness corneal laceration without uveal repositioning; and (v) anterior vitrectomy for removal of vitreous in anterior chamber. Code all procedures.
Diagnosis Codes
- S05.52xA Penetrating wound with foreign body, left eye
- H.26.102 Traumatic cataract, left eye
- S05.32xA Ocular laceration without prolapse or loss of intraocular tissue, left eye
Tips
- Trauma cases are inherently unique and thus require an individualized approach to coding.
- For removal of intraocular foreign bodies, always distinguish between magnetic and nonmagnetic for both the CPT and ICD-10-CM codes.
- For repair of corneal/scleral lacerations, the code choice is between whether or not there was prolapse of uveal tissue.
- Follow CPT guidelines when coding for lensectomy when performed with PPV: use 66850 and not 66852.2
- Chapter 20. External Causes of Morbidity (V00 – Y99) of ICD-10-CM is where one finds all the other miscellaneous codes caused by environmental events and circumstances. Happily, its use is not mandatory on a national requirement basis; however, ICD-10-CM cautions that there may by state-based reporting or individual payer mandate.
- Both an anterior vitrectomy for removal of vitreous present in the anterior chamber (CPT code 67010 for its removal mechanically) and a posterior vitrectomy were performed; however, because the two codes are bundled under the National Correct Coding Initiative, it is wisest not to code for the anterior vitrectomy, which would entail breaking the bundle.n
1. Asbell RL. Coding for surgical procedures in the global period. Retina Today. 2014;9(6):35-37.
2. Asbell RL. Solutions for a pair of puzzling surgical coding issues. Retina Today. 2015;10(3):31-33.
Riva Lee Asbell
• principal, Riva Lee Asbell Associates, in Fort Lauderdale, Fla.
• financial interest: none acknowledged
• rivalee@rivaleeasbell.com
• CPT codes copyright 2015 American Medical Association




_1784132761.jpg?auto=compress,format&w=75)











