


CASE REPORT
AT A GLANCE
• Metastasis to the retina and vitreous should be included in the differential diagnosis of patients with known or suspected malignancy who present with diffuse retinal vasculitis and vitritis.
• Retinal metastasis linked to systemic malignancy is often misdiagnosed and treated as infectious or inflammatory retinitis.
• Most cases of retinal metastasis are associated with a poor systemic prognosis.
A 51-year-old white woman presented with an 8-week history of blurry vision and floaters in her right eye (OD). She had a history of squamous cell carcinoma of the lung diagnosed 2 years prior to presentation. She had undergone radiation and chemotherapy and was in remission, but she was currently smoking and had chronic obstructive pulmonary disease, coronary artery disease, and hypertension. She reported no prior ocular disease.
Upon examination, the patient’s visual acuity was 20/63 OD and 20/20 in the left eye (OS). Intraocular pressure and slit-lamp examination were normal. Dilated fundus examination OD showed white deposits in the posterior vitreous and hyaloid, optic disc edema, diffuse retinitis, vascular sheathing, and perivascular infiltrates (Figure 1A, B, C). Fluorescein angiography OD confirmed retinal vasculitis and ischemia (Figure 1D, E, F). Fundus examination and angiography OS were normal. Clinical laboratory tests revealed elevated serum Toxoplasma and Toxocara IgG (negative IgM); nonreactive fluorescent treponemal antibody; negative tuberculosis gamma-interferon assay; and normal angiotensin converting enzyme and lysozyme.
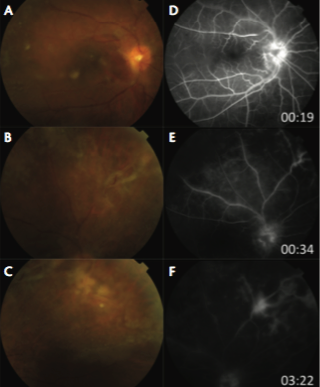
Figure 1. Clinical features. Dilated fundus examination OD showed mild vitritis, multiple white deposits in the posterior vitreous, diffuse whitening of the posterior hyaloid with ERM formation, mild optic disc edema with prepapillary vitreous deposits (A); retinal vascular sheathing with retinal necrosis and large inflammatory precipitates along retinal vessels, especially superonasally and nasally (B); superonasal tractional retinal detachment, and scattered areas of retinitis involving nasal, superior, and temporal periphery (C). Fluorescein angiography OD during laminar (D), venous (E), and late (F) phases showed leakage from the optic disc, leakage from retinal vessels, and staining of vessel walls consistent with retinal vasculitis mainly involving the venules, a focal area of intense hyperfluorescence superonasal to the disc consistent with focal retinitis, and patchy areas of capillary nonperfusion peripherally.
The patient was treated with oral clindamycin followed by prednisone for presumed ocular toxoplasmosis. At 1 month, there was no clinical improvement. At 2 months, there was clinical deterioration with anterior uveitis, increased vitritis, and vitreous opacities. Pars plana vitrectomy, epiretinal membrane (ERM) peeling, endolaser, and intravitreal injection of clindamycin, vancomycin, amikacin, and voriconazole were performed. Gram stain, cytomegalovirus polymerase chain reaction (PCR), varicella zoster PCR, herpes simplex virus 1 and 2 PCR, and bacterial and fungal cultures of vitreous specimen were negative. Papanicolaou-stained liquid-based cytology (Figure 2A) and hematoxylin and eosin–stained histologic preparation (Figure 2B) from the ERM specimen showed dysplastic squamous cells. Immunohistochemical stains of the ERM were positive for tumor protein p63 (Figure 2C) and negative for cytokeratin 7 and thyroid transcription factor-1. PET scan showed recurrent lung cancer.
Based on these analyses, lung carcinoma metastasis to the retina and vitreous was diagnosed. After vitrectomy, recurrence of retinitis and preretinal opacities from residual metastasis were observed. The patient refused additional treatment. After being lost to follow-up for 2 years, she returned with visual acuity of counting fingers OD, rubeosis iridis, and recurrent preretinal lesions and perivascular sheathing.
DISCUSSION
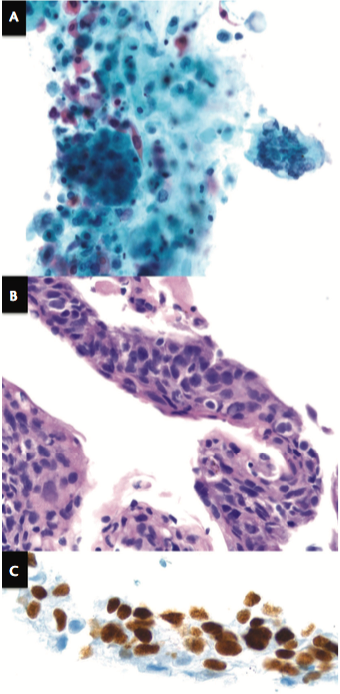
Figure 2. Histopathologic features. Papanicolaou-stained liquid-based cytology preparation (A) of the ERM specimen (original magnification 20X) showed keratinizing squamous cells with nuclear irregularity, pleomorphism, atypia, hypercellularity, and hyperchromasia. Hematoxylin and eosin–stained section (B) of the ERM (original magnification 40X) demonstrated severely dysplastic keratinizing cells with nuclear irregularity and mitoses, consistent with squamous cell carcinoma. Immunohistochemical staining (C) of ERM (magnification 100X) showed positive tumor protein p63 immunoperoxidase staining suggestive of squamous cell origin.
Metastasis to the retina and vitreous may masquerade as a diffuse retinal vasculitis and vitritis and should be included in the differential diagnosis of patients with known or suspected malignancy who present with such findings. Retinal metastasis from systemic malignancy is most commonly misdiagnosed and treated initially as an infectious or inflammatory retinitis.1,3
In this case, presence of serum Toxoplasma antibodies added to the diagnostic confusion, but vitrectomy with cytology and histopathology aided in establishing the correct diagnosis. Most cases of retinal metastasis are treated with observation, enucleation, or radiotherapy and are associated with a poor systemic prognosis.1 Despite her poor prognosis, the patient in this case is alive 2 years after her ocular diagnosis.1
CONCLUSION
Retinal metastasis from squamous cell carcinoma of the lung is exceedingly rare. It may present as focal or extensive retinal whitening with intraretinal or preretinal hemorrhages, and it is usually restricted to the inner retina.1,3,4 Vitreous seeding may accompany retinal metastasis.1,4 Isolated metastasis to the vitreous without a distinct retinal tumor has been previously reported.5,6 Jaissle et al studied vitreous metastasis from cutaneous melanoma and proposed that retrohyaloidal metastasis adjacent to an epiretinal hemorrhage may act as an access point for the intravascular melanoma cells to enter the vitreous cavity, followed by proliferation in the posterior vitreous as cellular aggregates, resulting in dense infiltration of the entire vitreous cavity.6 The clinical appearance in this case was unique with regard to absence of any retinal hemorrhage and predominance of a diffuse retinal vasculitis with vitritis. To the best of our knowledge, retinal and vitreous metastasis from lung cancer presenting with these simultaneous findings has not been previously described. n
1. Shields CL, McMahon JF, Atalay HT, et al. Retinal metastasis from systemic cancer in 8 cases. JAMA Ophthalmol. 2014;132(11):1303-1308.
2. Zografos L, Mirimanoff RO, Angeletti CA, et al. Systemic melanoma metastatic to the retina and vitreous. Ophthalmologica. 2004;218(6):424-433.
3. Payne JF, Rahman HT, Grossniklaus HE, Bergstrom CS. Retinal metastasis simulating cytomegalovirus retinitis. Ophthalmic Surg Lasers Imaging. 2012;43:e90-93.
4. Takagi T, Yamaguchi T, Mizoguchi T, Amemiya T. A case of metastatic optic nerve head and retinal carcinoma with vitreous seeds. Ophthalmologica. 1989;199(2-3):123-126.
5. Latkany P, Ciulla TA, Younger C, Gao H. Nonsmall cell lung adenocarcinoma metastatic to the vitreous without fundus lesions. Ophthalmic Surg Lasers. 2000;31(2):155-156.
6. Jaissle GB, Szurman P, Rohrbach JM, et al. A case of cutaneous melanoma metastatic to the vitreous cavity: possible pathomechanism and review of the literature. Graefes Arch Clin Exp Ophthalmol. 2007;245(5):733-7340.
Ramana S. Moorthy, MD
• associate clinical professor, department of ophthalmology, Indiana University School of Medicine, and founding partner of Associated Vitreoretinal and Uveitis Consultants, both in Indianapolis, Ind.
• financial interest: none acknowledged
Ann T. Moriarty, MD
• ocular pathologist, AmeriPath Indiana, in Indianapolis, Ind.
• financial interest: none acknowledged
Sanket U. Shah, MD
• professor of ophthalmology, Wake Forest School of Medicine, Winston-Salem, North Carolina
• third-year resident at Eugene and Marilyn Glick Eye Institute, department of ophthalmology, Indiana University School of Medicine, in Indianapolis, Ind.
• sanket1311@yahoo.com




_1784132761.jpg?auto=compress,format&w=75)











