
The use of lasers in surgical settings has undergone an evolution since their introduction. In the first generation of lasers, the instruments were so large they filled entire rooms and required specialized cooling systems. Many other iterations of laser systems for use in retinal surgeries have ensued, such as the safe and effective argon laser developed by Gholam Peyman, MD.1 Smaller, more portable systems such as diode lasers were later developed, allowing their transportation from site to site. Steve Charles, MD, introduced the concept of endophotocoagulation for vitreoretinal surgery, for which he first used a fiber optic probe attached to a portable xenon arc photocoagulator.2 This concept was later adapted for use with lasers, including argon and diode lasers.3
AT A GLANCE
• The number and types of laser probes have increased in recent years; they include straight, curved, blunt, tapered, aspirating, and illuminating options.
• Cannula designs have also changed and improved, as evidenced by the development of valved cannulas.
• With the A&I XR laser probe, surgeons can treat areas that have until now been difficult to access.
MORE PROBE CHOICES
As surgical systems have evolved, there has been a transition in laser probes as well. With the advent of smaller gauge systems, the number and types of available probes have increased. From straight, curved, blunt, and tapered, to aspirating and illuminating probes, the choices now are many. Recently, with the rise of microincisional surgical techniques, 23-gauge and 25-gauge probes have become available.
A probe I have found particularly effective is the Adjustable and Intuitive Extended Reach (A&I XR) probe (Iridex). This extendable retinal probe can be altered from straight to curved at the touch of a button (Figure). It offers increased extension and a greater curvature than previous A&I standard models (Iridex), enabling treatment more anteriorly. The device also allows uninterrupted adjustment of the fiber optic over a greater angular range than previous models, permitting the surgeon to fully cover the peripheral retina without removing the probe from the eye. Enhancements to the technology have created a tighter laser cone angle that enables the surgeon to treat at a greater distance from the retina and aids in conserving laser power density, thus facilitating safer and more controlled procedures.4
Although there is no miracle probe available that will work for every situation and every patient, in my experience this probe provides superior access to problematic areas. I have found that, in conjunction with valved cannulas, the 25-gauge A&I XR probe fits all of my requirements, eliminating the need for different gauges of straight- and curved-tipped probes.
THE ERA OF THE VALVED CANNULA
In parallel with recent improvements in laser probe technology, advances in cannula design have brought about the development of valved cannulas. Valved cannulas provide the surgeon with a greater degree of control than nonvalved cannulas, minimizing fluid egress around the cannula and thereby aiding in controlling intraocular pressure (IOP). The cannulas act as a self-sealing system, preventing undesired fluid exchange and maintaining a stable IOP while reducing bleeding and other potential complications.
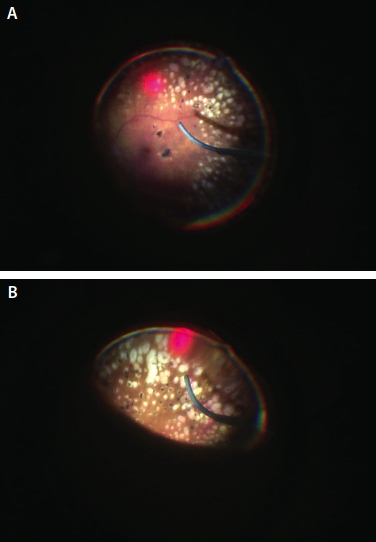
Figure. The A&I XR probe can be altered from straight to curved at the touch of a button, allowing the surgeon to fully cover the peripheral retina without removing the probe from the eye. Probe fully extended, demonstrating its curvature (A). Probe in extended reach position; far peripheral location (B).
Prior to the availability of valved cannulas, it was necessary to use a laser probe that fit the diameter of the cannula being used in a particular surgery. Therefore, it was essential to maintain a stock of multiple gauge sizes and different types of laser probes to be prepared for what might be needed in the OR. Often, much of this stock would go to waste through error when one surgical pack was selected in place of another or through expiration. This waste could be expensive, but it was necessary because there were no other options. Thankfully this is no longer the case, as valved cannulas allow the surgeon to choose one probe and use it on all cases.
I use the 25-gauge A&I XR probe with the 532-nm OcuLight GLx (Iridex) laser. Hard dollars, such as the cost per unit to purchase a product, are easy to measure. Soft dollars, such as the expense of performing inventory control, creating shelf space, or opening the incorrect item, are not as simple to determine but are just as real as hard expenses. The adjustable probe has a more expensive per-unit cost than standard probes, but using one type of probe for every procedure results in minimizing space on the stock shelf, saving inventory, and reducing or eliminating waste through expired merchandise. A one-size-fits-all approach simplifies OR and inventory room functions, and, in the long run, reduces soft dollar expenses.
Do not get lost in hard dollar costs. Be aware of what is being lost when there is bleeding of soft dollars—whether in your practice, hospital, or ambulatory surgery center. Standardization of surgical equipment such as laser probes can help lead to cost savings and greater surgical efficiency.
INVEST IN QUALITY
Technology continues to advance, providing ever-improving instrumentation that both simplifies treatment and addresses cost issues. The A&I XR laser probe offers the ability to treat areas that have until now been difficult to access. Using these probes with valved cannulas eliminates the need to stock multiple sizes and types of probes, which reduces waste, ultimately lowers overhead, potentially decreases mistakes, and creates greater efficacy and control through the entire surgical process. n
1. Peyman GA, Grisolano JM, Palacio MN. Intraocular photocoagulation with the argon krypton laser. Arch Ophthalmol. 1980;98:2062-2064.
2. Charles S. Endophotocoagulation. Retina. 1981;1:117-120.
3. Fleischman JA, Swartz M, Dixon JA. Argon laser endophotocoaguation: An intraoperative trans-pars-plana technique. Arch Ophthalmol. 1981;99(9):1610-1612.
4. Whitacre MM, Timberlake GT, Stein RA, Stanley AM, Van Vleck S, Dominick KE. Light distribution of ocular endophotocoagulator probes and its surgical implications. Lasers Surg Med. 1994;15:62-73.
Section Editor Dean Eliott, MD
• associate director, retina service, Massachusetts Eye and Ear,
Boston, Mass.
Section Editor Ingrid U. Scott, MD, MPH
• professor of ophthalmology and public health sciences, Penn
State Eye Center, Penn State College of Medicine, Hershey, Pa.
R. Mark Hatfield, MD, FACS
•founder, Retina Consultants PLLC in Charleston, W. Va.
•financial interest: none acknowledged
•retinaconwv@msn.com






_1784132761.jpg?auto=compress,format&w=75)











