

Acute lymphoblastic leukemia (ALL) is the most common type of cancer in children in the United States. Nowadays, chemotherapy regimens are risk-adapted according to clinical and genetic features.1,2 Any acute leukemia can affect the eye by infiltration of tissues (around retinal vessels, choroid, and optic nerve), intraocular hemorrhagic events, or a combination of both. A highly elevated leukocyte count causes the former, and the hemorrhagic episodes tend to appear when anemia or thrombocytopenia are present.3 Any intraocular hemorrhage in children may permanently affect vision if rehabilitation is not initiated before amblyopia occurs. Pars plana vitrectomy has led to good anatomical and functional results when spontaneous resolution of the hemorrhage is not achieved,4,5
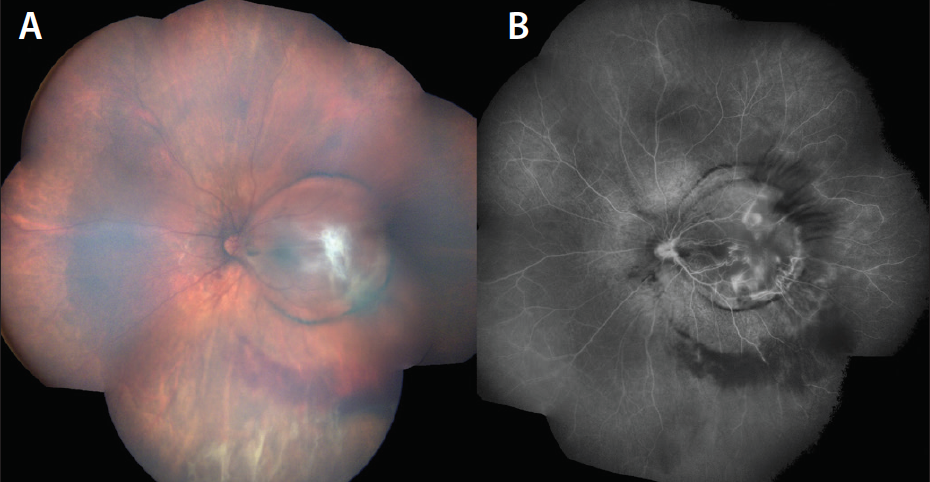
Figure 1. Clinical photograph and FA before surgery. On the left (A), the composed ultra-widefield color photo shows inferior vitreous hemorrhage, preretinal fibrosis at the macula, and a macular dome-shaped lesion with a pigmented demarcation line. FA on the right (B) shows blockage of fluorescence secondary to the blood, with hyperfluorescent staining of the fibrous material and vascular leakage.
We present a case of a pediatric patient with ALL and Terson syndrome. She had very low blood counts at presentation, but was referred to Bascom Palmer Eye Institute after her ALL was stabilized. A 27-gauge pars plana vitrectomy was performed as part of her visual rehabilitation therapy with good functional results.
Case Report
A 4-year-old girl was diagnosed with ALL, severe anemia, and thrombocytopenia. She had a positive TEL-AML1 gene profile (a marker of low-risk disease) and was undergoing a strict risk-adapted chemotherapy regimen.1,2
During treatment, the patient had an intracranial hemorrhage with no central sequelae, after which her parents noted vision loss. Thirteen months after the initial diagnosis, she was referred to a retina specialist for evaluation with a diagnosis of possible neoplastic ocular infiltration of the left eye at the macula. The patient was undergoing maintenance therapy after remission.
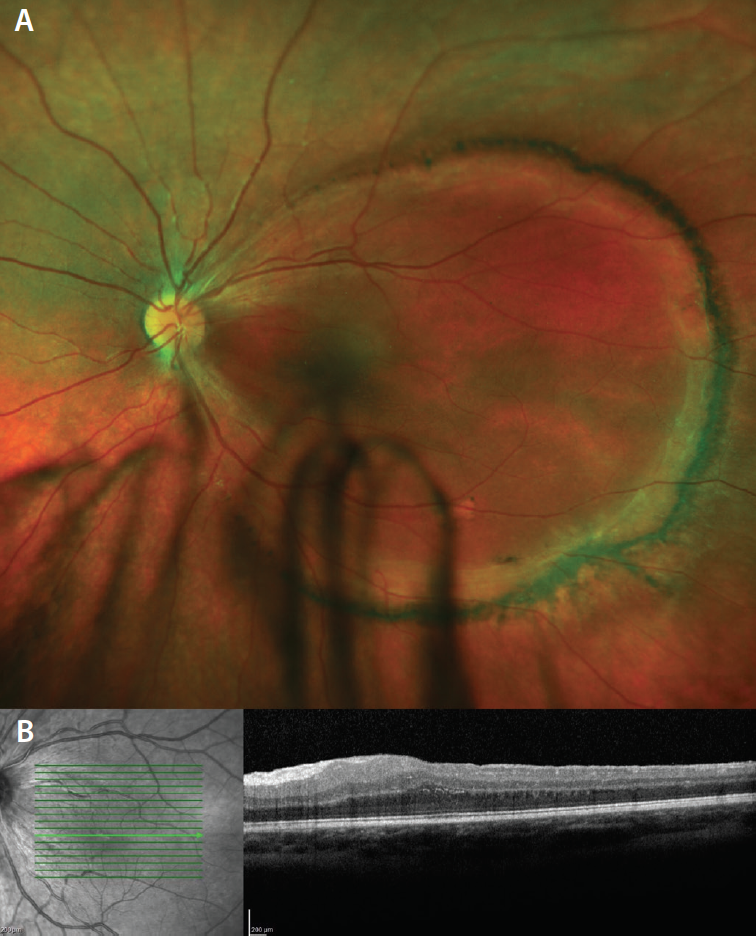
Figure 2. Five months after surgery. (A) An attached retina with a pigmented ring at the posterior pole is seen on the superior color image. Optical coherence tomography (B) shows absence of foveal contour with presence of inner retina layers and a visible photoreceptor layer.
Best corrected visual acuity (BCVA) was 20/20 in the right eye and hand motion in the left eye. The right eye was unremarkable, while the left eye showed a vitreous hemorrhage with an elevated round lesion at the macula, preretinal fibrous tissue, and a demarcation line. Fluorescein angiography was performed during an examination under anesthesia (Figure 1).
A 27-gauge pars plana vitrectomy was performed on the left eye to remove the vitreous hemorrhage and the premacular dome-shaped lesion, followed by endolaser and 16% SF6 as tamponade. Twenty-nine months after the surgery, the BCVA of the left eye is 20/60 with refractive correction and right eye patching a few hours a day (Figure 2).
Discussion
Acute leukemia can present with a wide array of manifestations in the retina that are not always diagnosed, although there is evidence of it on histopathological studies. The treating physician must remain alert to any sign of ocular involvement because recurrent leukemia can manifest initially in the eye. Most importantly, when the eye is affected, the central nervous system can be compromised, thus clinical suspicion is crucial and prompt ophthalmological evaluation is required.3,6
Although rare in children, Terson syndrome occurs when intraocular hemorrhage appears at the same time as intracranial bleeding secondary to trauma, ruptured aneurysms, or hematological disorders.7-10 Resultant severe pancytopenia from acute leukemia predisposes the patient to any type of bleeding in the body.9 Two clinical findings support the diagnosis of Terson syndrome in our case: the retinal hemorrhage on Terson’s tends to be localized and posterior; and according to Srinivasan et al., a “double ring” is seen with an ILM hemorrhage (inner ring) and a subhyaloid bleed (outer ring).7-9,11
The objective of the surgery is to clear the visual axis after ruling out that the vision loss is not a result of central nervous system damage.5 Narayanan et al., reported visual acuities after vitrectomy in adults that did not improve spontaneously after Terson syndrome. They demonstrated final visual acuities of 20/50 or better. These results can be extrapolated to children if no additional intrinsic retinal damage is found and prompt surgery is offered. It is important to complete rehabilitation with spectacle correction and proper amblyopia management.4,9
Summary
Acute leukemia in children can have serious ocular manifestations that physicians must have in mind at all times during treatment and long-term follow up. Retinal hemorrhages that affect the visual axis should be treated promptly. Pars plana vitrectomy in children with endotamponade is a good option as part of the early visual multidisciplinary rehabilitation. n
Editorially independent supported by advertising from Alcon and Topcon.
1. National Cancer Institute. Risk-Adapted Chemotherapy in Treating Younger Patients with Newly Diagnosed Standard-Risk Acute Lymphoblastic Leukemia or Localized B-Lineage Lymphoblastic Lymphoma. https://www.cancer.gov/about-cancer/treatment/clinical-trials/search/view?cdrid=683227. Accessed July 22, 2017.
2. Zelent A, Greaves M, Enver T. Role of the TEL-AML1 fusion gene in the molecular pathogenesis of childhood acute lymphoblastic leukaemia. Oncogene. 2004;23:4275-4283.
3. Robb RM, Ervin LD, Sallan SE. A pathological study of eye involvement in acute leukemia of childhood. Trans Am Ophthalmol Soc. 1978;76:90-101.
4. Narayanan R, Taylor SC, Nayaka A, et al. Visual outcomes after vitrectomy for Terson syndrome secondary to traumatic brain injury. Ophthalmology. 2017;124:118-122.
5. Mills MD. Terson syndrome. Ophthalmology. 1998;105:2161-2163.
6. Patel AV, Miller JB, Nath R, et al. Unilateral eye findings: a rare herald of acute leukemia. Ocul Oncol Pathol. 2016;2:166-170.
7. Bhardwaj G, Jacobs MB, Moran KT, Tan K. Terson syndrome with ipsilateral severe hemorrhagic retinopathy in a 7-month-old child. J AAPOS. 2010;14:441-443.
8. Parsons SR, Qiu M, Han IC. Terson syndrome from subarachnoid hemorrhage in aplastic anemia. Ophthalmology. 2016;123:1035.
9. Lorenzi U, Buschini E, Fea A, Machetta F, Grignolo FM. Terson syndrome and leukemia: a case report. Clin Ophthalmol. 2014;8:681-683.
10. Scheller J, Doroslovacki P. Ruptured aneurysm and Terson syndrome in a 1-month-old infant. Pediatr Neurol. 2015;52:653-654.
11. Srinivasan S, Kyle G. Subinternal limiting membrane and subhyaloid haemorrhage in Terson syndrome: the macular ‘double ring’ sign. Eye (Lond). 2006;20:1099-1101.
Audina M Berrocal, MD
• professor of clinical ophthalmology at the Bascom Palmer Eye Institute, Miami, FL
• medical director of Pediatric Retina and Retinopathy of Prematurity at the Bascom Palmer Eye Institute, Miami, FL
• vitreoretinal fellowship co-director at the Bascom Palmer Eye Institute, Miami, FL
• member of the Retina Today editorial board
• consultant to Alcon, Dutch Ophthalmic Research Center, and Visunex Medical Systems
• aberrocal@med.miami.edu
Linda A Cernichiaro-Espinosa, MD
• vitreoretinal surgeon
• international pediatric retina fellow at the Bascom Palmer Eye Institute, Miami, FL
• No financial/conflicting interest to disclose
• linda.cernichiaro@gmail.com
_1784132761.jpg?auto=compress,format&w=75)











