Asubmacular hemorrhage can have devasting consequences for vision with irreversible destruction of photoreceptors within 24 hours.1 Research shows that 60% of submacular hemorrhage cases in Asia are caused by polypoidal choroidal vascularization (PCV).2 This condition is more prevalent in Black and Asian populations (predominantly Japanese) compared with the White population.3
Because treatment of submacular hemorrhage with displacement techniques is more successful when the blood clot has not organized, prompt referral is crucial. Generally, the patient notes a central scotoma, and the hemorrhage is readily apparent on examination. Physicians should suspect a submacular hemorrhage in patients with a history of AMD or PCV who present with an acute loss of central vision.
CURRENT OPTIONS
Surgeons often turn to one of three management strategies for submacular hemorrhage:
- Pneumatic displacement with an intravitreal expansile gas bubble injection either alone or in combination with intravitreal tissue plasminogen activator (tPA);4,5
- Vitrectomy and subretinal injection of tPA followed by tamponade with air or an expansile gas; or5-10
- Retinotomy and manual removal of the subretinal clot in cases of massive subretinal hemorrhage followed by silicone oil tamponade.11
Of these options, intravitreal injection of expansile gas and tPA has the advantage of being simple and cost effective. In more complex cases we prefer performing a vitrectomy and injecting subretinal tPA followed by tamponade with an expansile gas. In the latter approach, injecting the tPA subretinally in a controlled manner can be challenging.
In the past, we used a 1-cc syringe connected to a 25-gauge subretinal cannula for subretinal tPA injection. For this procedure, the surgeon held the syringe while the assistant depressed the plunger. This method often resulted in an uncontrolled flow of fluid into the subretinal space and was dependent on the steadiness of the assistant’s hand.
Specialized equipment for subretinal injection, such as the MicroDose injection kit (MedOne Surgical), has been developed. However, this product is not marketed or approved in Indonesia, and if it were, it would likely increase the expense of surgery. Novelli et al recently reported a novel method in which an insulin syringe with a 41-gauge cannula coupled with the viscous fluid control unit of a standard vitrectomy system is used for subretinal tPA injection.9 We were also looking for a more efficient method, and we developed a simpler and more cost-effective method using the materials supplied with standard vitrectomy packs.

Preparing Subretinal tPA Injection
A NEW APPROACH
In our approach, 0.2 cc of the tPA alteplase (Actilyse, Boehringer Ingelheim) is injected into one end of an infusion extension tube. The same end of the tube is connected to a subretinal cannula, and the other end to a 10-cc syringe supplied with the Viscous Fluid Control Pak injection system for the Constellation Vision System (Alcon; Figures 1 and 2).
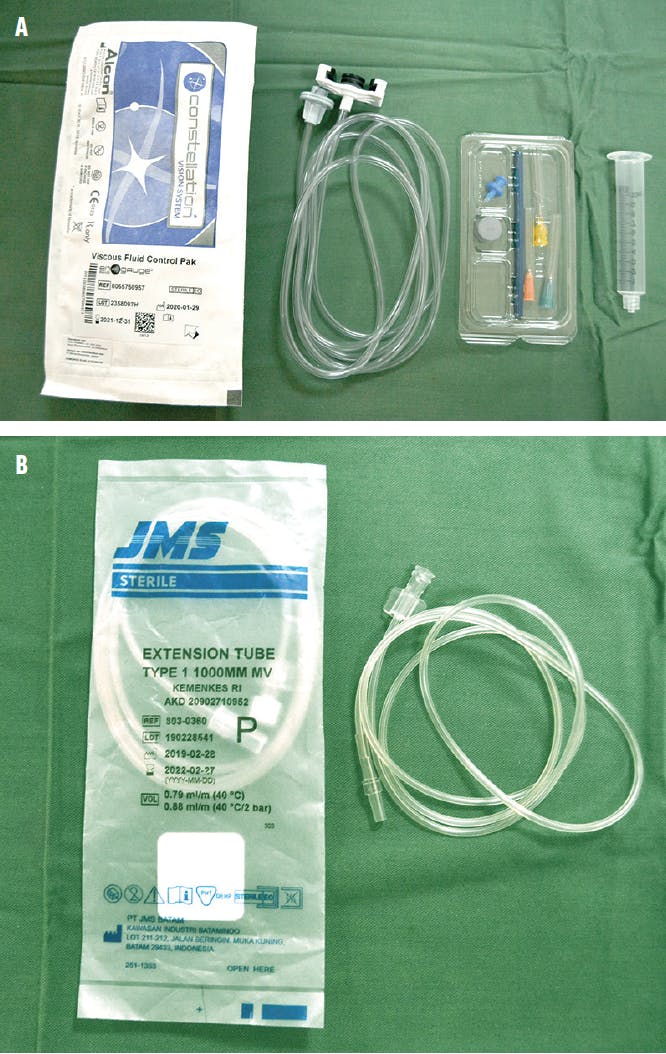
Figure 1. The authors’ method uses the Alcon Viscous Fluid Control Pak (A) and 1-mm diameter extension tubing (B).

Figure 2. tPA is injected into one end of the extension tubing (A), after which a subretinal cannula is attached (B).
The pressure of the viscous fluid injection is lowered to between 4 psi and 8 psi, which is enough to allow controlled flow of the solution through the subretinal canula. The surgeon can adjust the speed of injection using the footpedal.
When the footpedal is depressed, the plunger of the 10-cc syringe moves slightly forward, flushing the alteplase through the extension tubing into the subretinal cannula.
In some cases, the surgeon may choose to inject a subretinal air bubble before the alteplase is injected; to do this, the surgeon can aspirate a small amount of air into the infusion line ahead of the alteplase.
One possible complication is the risk of injecting too much fluid too quickly into the subretinal space, causing the injected fluid to burst through the macula.

Subretinal tPA Injection
CLINICAL PERSPECTIVE
All previous patients were injected manually with difficulty keeping the flow steady, and we did not dare inject in more than one site for fear of causing a complication. We have used this new method on three patients with good results. Here are the clinical outcomes of two of them:
A 64-year-old woman presented with a sudden decrease in vision in the right eye from 1.0 to 0.2 based on the ETDRS protocol. She had a history of PCV and multiple injections of aflibercept (Eylea, Regeneron) in the right eye, and her left eye is blind. She had a submacular bleed involving the fovea. We performed a 25-gauge vitrectomy with subretinal alteplase injection followed by tamponade with SF6 gas (Figure 3). Vision has improved slightly to 0.3.

Figure 3. Before (A) and after (B) displacement of a patient’s submacular hemorrhage with subretinal alteplase injection.

Figure 4. Before (A) and 3 weeks after (B) displacement of a patient’s submacular hemorrhage with subretinal tPA with gas tamponade.
A 61-year-old man presented with sudden loss of vision to counting fingers in the left eye. His examination revealed a large subretinal hemorrhage involving the macula. We performed a 25-gauge vitrectomy with subretinal injection of alteplase in three different areas followed by tamponade with SF6 gas. Three weeks after displacement, vision had improved to 0.8 (Figure 4).
1. Glatt H, Machemer R. Experimental subretinal hemorrhage in rabbits. Am J Ophthalmol. 1982;94(6):762-773.
2. Kunavisarut P, Thithuan T, Patikulsila D, et al. Submacular hemorrhage: visual outcomes and prognostic factors. Asia-Pacific J Ophthalmol. 2018;7(2):109-113.
3. Palkar AH, Khetan V. Polypoidal choroidal vasculopathy: An update on current management and review of literature. Taiwan J Ophthalmol. 2019;9(2):72-92.
4. Chen CY, Hooper C, Chiu D, Chamberlain M, Karia N, Heriot WJ. Management of submacular hemorrhage with intravitreal injection of tissue plasminogen activator and expansile gas. Retina. 2007;27(3):321-328.
5. Hillenkamp J, Surguch V, Framme C, Gabel VP, Sachs HG. Management of submacular hemorrhage with intravitreal versus subretinal injection of recombinant tissue plasminogen activator. Graefes Arch Clin Exp Ophthalmol. 2010;248(1):5-11.
6. Haupert CL, McCuen BW 2nd, Jaffe GJ, et al. Pars plana vitrectomy, subretinal injection of tissue plasminogen activator, and fluid-gas exchange for displacement of thick submacular hemorrhage in age-related macular degeneration. Am J Ophthalmol. 2001;131(2):208-215.
7. Olivier S, Chow DR, Packo KH, MacCumber MW, Awh CC. Subretinal recombinant tissue plasminogen activator injection and pneumatic displacement of thick submacular hemorrhage in age-related macular degeneration. Ophthalmology. 2004;111(6):1201-1208.
8. Bell JE, Shulman JP, Swan RJ, Teske MP, Bernstein PS. Intravitreal versus subretinal tissue plasminogen activator injection for submacular hemorrhage. Ophthalmic Surg Lasers Imaging Retina. 2017;48(1):26-32.
9. Novelli FJD, Preti RC, Monteiro MLR, Nobrega MJ, Takahashi WY. A new method of subretinal injection of tissue plasminogen activator and air in patients with submacular hemorrhage. Retina. 2017;37(8):1607-1611.
10. Kimura S, Morizane Y, Hosokawa MM, et al. Outcomes of vitrectomy combined with subretinal tissue plasminogen activator injection for submacular hemorrhage associated with polypoidal choroidal vasculopathy. Jpn J Ophthalmol. 2019;63(5):382-388.
11. Isizaki E, Morishita S, Sato T, et al. Treatment of massive subretinal hematoma associated with age-related macular degeneration using vitrectomy with intentional giant tear. Int Ophthalmol. 2016;36(2):199-206.



_1784132761.jpg?auto=compress,format&w=75)











