


A 41-year-old patient presented to our clinic with painless loss of vision in each eye for the last 2 weeks. BCVA was 6/60 OD and counting fingers OS. The anterior segment examination was normal. Fundus examination of the right eye showed disc hyperemia with marked yellowish-white choroidal plaque-like lesions over the posterior pole with retinal periphlebitis and vitreous bead-like opacities (Figure 1, A). The left eye showed marked disc edema with choroidal lesions along the arcade blood vessels and peripheral vessel sheathing (Figure 1, B). Fluorescein angiography (FA) and OCT confirmed the active chorioretinitis lesions along with disc leakage (Figure 2).

Figure 1. The right eye presented with disc hyperemia with yellowish-white choroidal plaque-like lesions over the posterior pole with retinal periphlebitis and vitreous bead-like opacities (A). The left eye showed disc edema with choroidal lesions along the arcade blood vessels and peripheral vessel sheathing (B).

Figure 2. FA of the left eye (A) showed disc leakage with well-defined staining of choroidal lesions (B, C) and vascular staining in the right eye (D). OCT of the left eye showed disc edema (E) and hyper-reflective dots at the subretinal and choroidal level (F).
The patient gave a history of high-risk sexual behavior and tested positive for human immunodeficiency virus (HIV)-1 (Western blot method) and syphilis (rapid plasma antigen in a dilution of 1:16 and treponema pallidum hemagglutination). These results confirmed a diagnosis of acute posterior placoid syphilitic chorioretinopathy. A cerebrospinal fluid (CSF) tap was also venereal disease research laboratory (VDRL) reactive.
The patient was admitted to the hospital and started on penicillin G injection at 24 million units daily for 14 days, along with highly active antiretroviral therapy. At 2 months follow-up, BCVA improved to 6/9 OD and 6/6 OS. The retinal lesions had healed completely with a leopard spot appearance, typical of ocular syphilis (Figure 3).
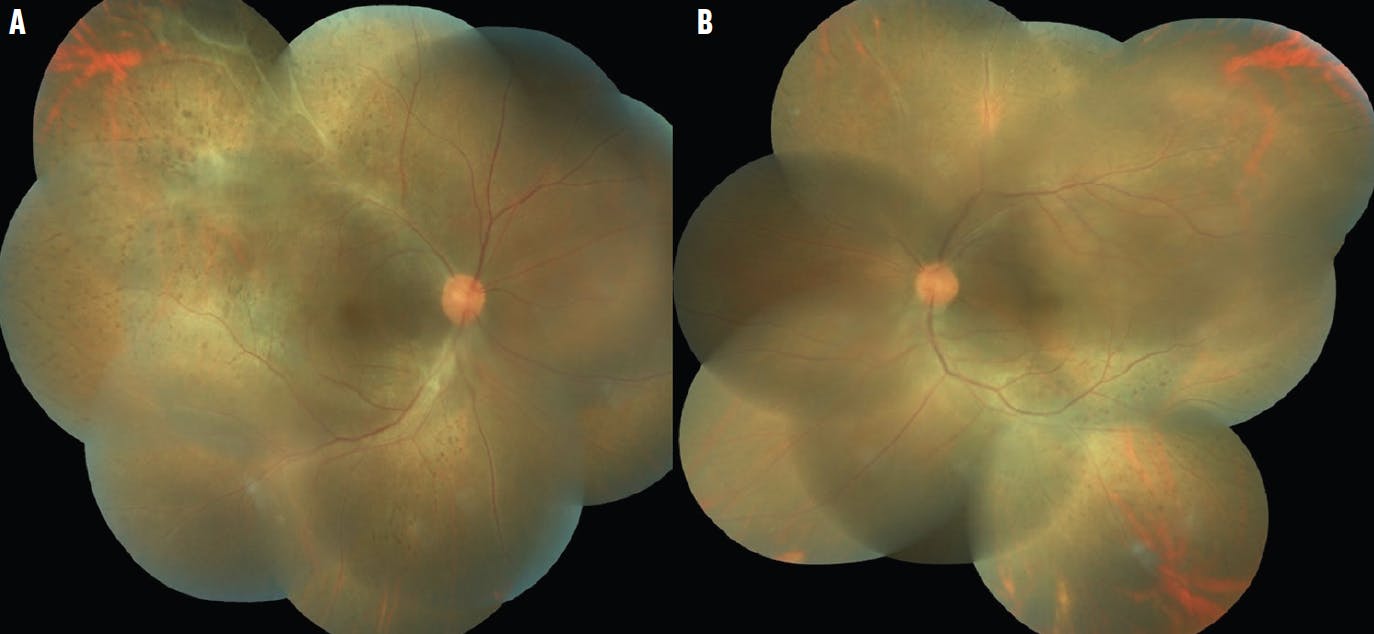
Figure 3. Fundus imaging of the right (A) and left (B) eyes after treatment showed typical leopard dot appearance.
DISCUSSION
Ocular syphilis can have myriad manifestations, with pan uveitis being the most common.1 Acute posterior placoid chorioretinopathy is a characteristic lesion of syphilis and is frequently seen in patients with secondary and late latent syphilis.2 This straightforward case of a rare entity brings several notable pearls to mind. First and foremost, early diagnosis and proper management can lead to improved visual outcomes, despite a dramatic presentation. Because there is an established high association of HIV with syphilis, concomitant testing is crucial.3 A CSF analysis for VDRL reaction and a fluorescent treponemal antibody test absorption test are also essential to rule out neurosyphilis. Partner education and testing for sexually transmitted diseases is of great importance.
If you have an image or images you would like to share, email Dr. Nagpal.
Note: Photos should be 400 dpi or higher and at least 10 inches wide.
1. Majumder PD, Chen EJ, Shah J, et al. Ocular syphilis: an update. Ocul Immunol Inflamm. 2017;27(1):117-125.
2. Woolston SL, Dhanireddy S, Marrazzo J. Ocular syphilis: a clinical review. Curr Infect Dis Rep. 2016;18(11):36.
3. Sudharshan S, Menia NK, Selvamuthu P, Tyagi M, Kumarasamy N, Biswas J. Ocular syphilis in patients with human immunodeficiency virus/acquired immunodeficiency syndrome in the era of highly active antiretroviral therapy. Indian J Ophthalmol. 2020;68(9):1897-1893.

_1784132761.jpg?auto=compress,format&w=75)











