

A 28-year-old female powerlifter presented to the clinic with 20/400 BCVA and a serous macular detachment secondary to an optic nerve pit (Figure 1). The detachment was severe enough to warrant vitrectomy in lieu of laser barricade, and I proceeded with surgery that included posterior hyaloid membrane stripping, ILM peeling, subretinal fluid drainage via a temporal macular retinotomy, endolaser, and a gas-fluid exchange. The patient’s anatomy appeared to recover in the postoperative period, but fluid recurred approximately 3 weeks after the resolution of the gas bubble, likely linked to the patient’s resumption of powerlifting. I elected to proceed with an amniotic membrane (AM) transplant. Both surgeries were done using the heads-up NGENUITY 3D Visualization System.
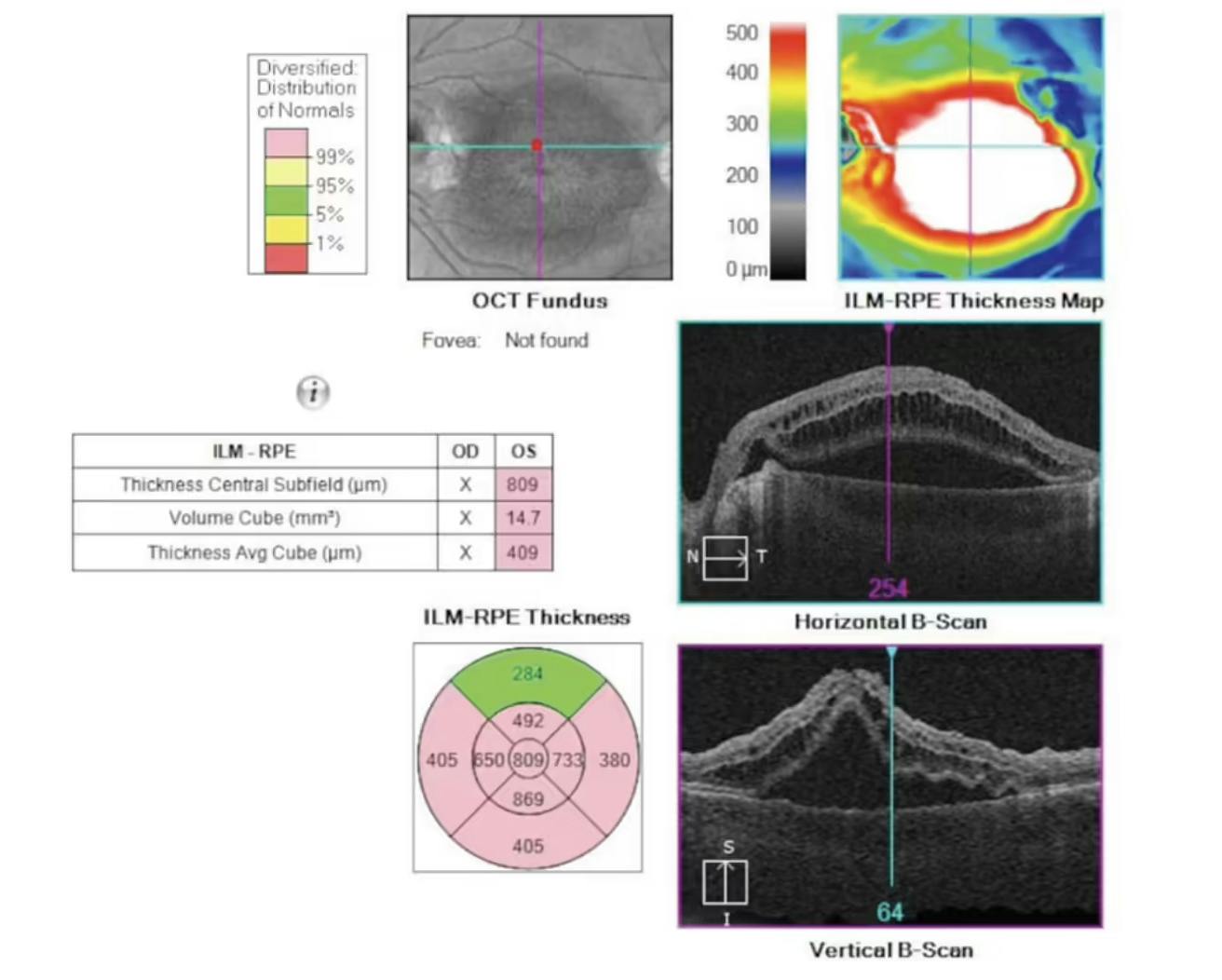
Figure 1. A serous macular detachment as depicted on preoperative imaging. The severity of the anatomy matched the patient’s decline in BCVA, which was measured at 20/400 upon presentation.
Placement of an AM presents a number of challenges. The stromal side of an AM is sticky, which makes it difficult to manipulate during surgery. Maintaining proper orientation, with the stromal side facing the host tissue, is of utmost importance. Although I was able to enter the eye with the AM grasped in GRIESHABER REVOLUTION DSP ILM Forceps (Alcon) via a valved-port with relative ease, I was unable to control the AM even when using the light pipe as a second instrument. The AM was so flimsy that even perfluorocarbon was unable to keep it controlled after placing it stromal-side down on the retina.
I proceeded with placing a chandelier light so I could employ a bimanual technique, allowing me to use the GRIESHABER MAXGRIP Forceps (Alcon) as a second instrument for optimizing my grasp on the AM (Figure 2). Using the forceps, I re-grasped the AM, which had adhered to the initial forceps. I then oriented the AM appropriately and slowly filled the surrounding area with perfluorocarbon until the globe was full.

Figure 2. After installing a chandelier light, the light pipe was swapped with GRIESHABER MAXGRIP Forceps. The AM was removed from the initial pair of forceps to which it had adhered. Use of perfluorocarbon then assisted in stabilizing the AM over the appropriate tissue area.
Imaging showed that fluid and the macular detachment had resolved at 1 week; as of 2 months’ follow-up, the patient’s anatomy remained intact as her functional vision improved. She has since returned to powerlifting and has not reported visual dysfunction or recurrence of fluid.

© 2023 Alcon Inc. 2/23 US-VIT-2300025