
The secret to streamlining retina coding is building foundational knowledge. Mastering key guidelines provides practitioners with a roadmap for efficient coding and reimbursement. This is especially true for the frequently provided services in the retina practice, which can require bundled current procedural terminology (CPT) codes, nuanced CPT codes, combined cases, and more. Thus, understanding the fundamental rules when coding these procedures can help you build expert knowledge. Let’s review five of these essential tricks of the trade.
1. REMEMBER THAT ALL VITRECTOMY CODES ARE BUNDLED
Retina surgical cases frequently incorporate multiple techniques to treat various pathologies. Along with pars plana vitrectomy (PPV), retina specialists can perform lasers, membrane peels, fluid-air exchange, and silicone oil tamponade. These procedures are reflected in the vitrectomy family of CPT codes 67036–67043 (Table 1).
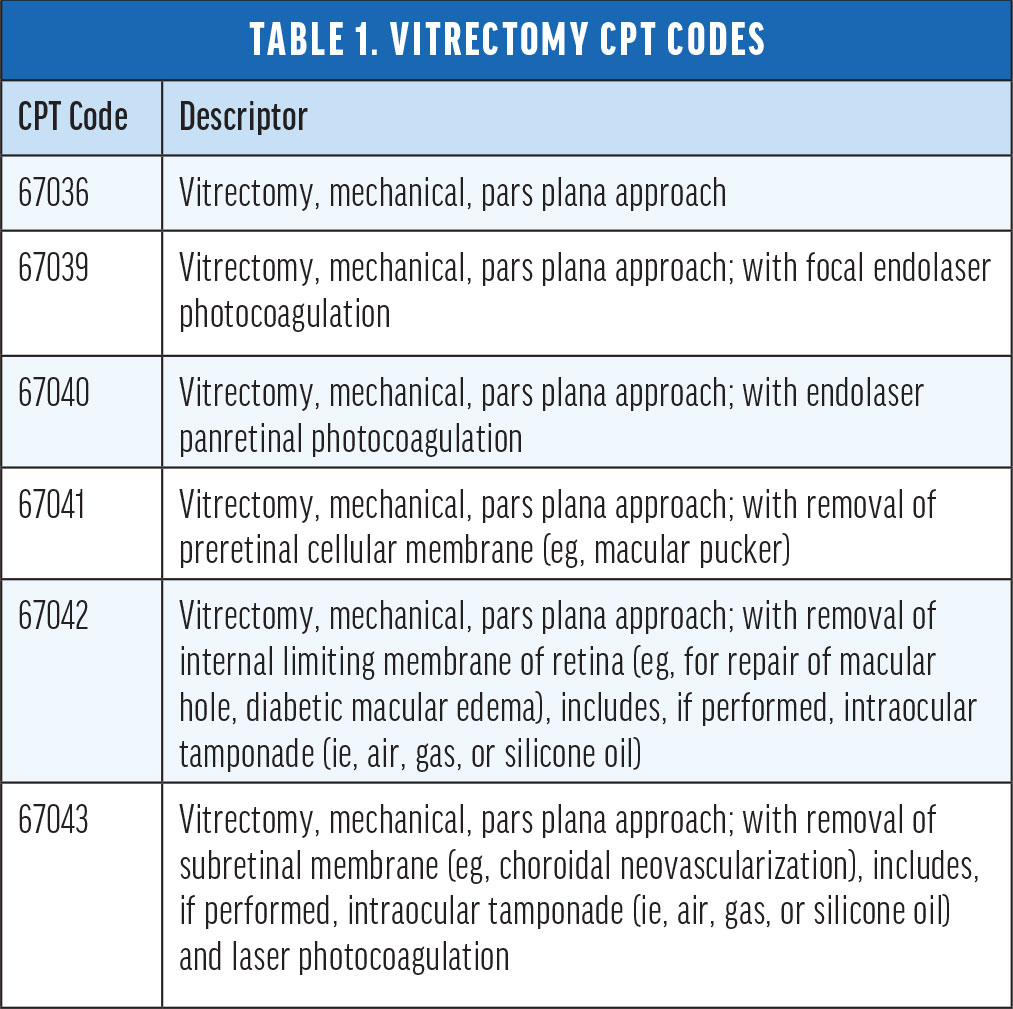
When reviewing the operative report, multiple vitrectomy CPT codes are commonly represented in the procedures performed. However, these codes are all bundled under National Correct Coding Initiatives (NCCI). It is not appropriate to unbundle when procedures were performed in the same eye and same structure (posterior segment).
For example, take a case where a PPV, endolaser panretinal photocoagulation, and membrane peel are performed. This procedure is represented by both CPT codes 67040 and 67041 but is bundled under NCCI. Providers should bill the CPT code with the highest relative value unit (RVU), which in this example is 67041.
Furthermore, CPT code 67121 (removal of implanted material, posterior segment; intraocular) is also bundled with the entire vitrectomy code family. If removing silicone oil, for example, CPT code 67121 represents this procedure; however, if a PPV was performed, report CPT code 67036, as it best represents the procedure performed.
2. CONFIRM THE DIAGNOSIS
When coding retina lasers or surgeries, the first step to correct coding is to confirm the diagnosis. While the same diode laser may be used in the clinic, the appropriate CPT code is determined by the reason for the procedure—not the laser itself.1 For example, when treating macular edema, the appropriate CPT code is 67210, destruction of localized lesion of retina (eg, macular edema, tumors, one or more sessions; photocoagulation). Also, repair of retinal detachment (CPT code 67105) by laser is reported differently than repair of a retinal tear (CPT code 67145).
Code selection for retinal surgical procedures is also determined by the diagnosis.2 For example, the CPT code for a PPV with a membrane peel and fluid-air exchange changes based on the diagnosis. If the diagnosis is a macular hole, the CPT code will be 67042. Alternatively, if the diagnosis is a tractional retinal detachment, the CPT code will be 67113, repair of complex retinal detachment (eg, proliferative vitreoretinopathy, stage C-1 or greater, diabetic tractional retinal detachment, retinopathy of prematurity, retinal tear of greater than 90°), with vitrectomy and membrane peeling, including air, gas, or silicone oil tamponade, cryotherapy, endolaser photocoagulation, drainage of subretinal fluid, scleral buckling, and/or removal of lens, when performed.
3. RECOGNIZE NUANCED CODING
When it comes to compounded bevacizumab (Avastin, Genentech/Roche), it’s important to recognize the nuanced coding involved, as the appropriate health care common procedure coding system (HCPCS) code will vary by insurance payer (Table 2).

Medicare administrative contractors (MACs) publish their guidance in local coverage determination (LCD) policies, local coverage articles (LCA), or bulletins.3 These MAC policies also vary; for example, Novitas requires J7999, while Palmetto expects J9035 when coding for bevacizumab.
Medicare Advantage, commercial, and Medicaid plans will not necessarily follow the local MAC guidelines. They often create their own policies for bevacizumab, which can also change periodically.
Although C9257 is intended for facility billing, some insurance payers have required this HCPCS code to report bevacizumab when performed in the office setting. If this is the preferred code, it is essential to report 5 units, as the code descriptor represents 0.25 mg as 1 unit. These units would accurately bill the 1.25 mg dosage for compounded bevacizumab.
To combat these variations, the best practice is to, first, embrace the fact that code selections vary, then identify the approved code for each of the payers. One great tip is to create an internal quick reference guide and provide this guidance to the entire practice team to ensure correct coding and reduce any claim denials.
4. IDENTIFY TESTING BUNDLES
There are multiple diagnostic testing services in a retina practice, often due to the medical necessity to perform them during the same encounter. Because of this, NCCI edits should be determined prior to claim submission.
Again, using a quick reference guide provides prompt decision making.4,5 The first step is to determine if the test is bundled and if the edit is considered comprehensive (indicator of 1) or mutually exclusive (indicator of 0). When mutually exclusive, the tests can never be unbundled with modifier –59, distinct procedural service. If a comprehensive edit applies, only unbundle the tests when the payer provides a published policy with guidance.
WPS Government Health Administrators LCD L34760 discusses the comprehensive bundle of CPT code 92134, OCT, and 92250, fundus photography.3 The guidance states that, generally, these two tests are bundled; however, infrequently, it may be medically necessary to unbundle the services when performed on the same day, and you must clearly document that to justify the decision. An example would be unique diagnoses for each test (eg, choroidal lesion for fundus photography and diabetic macular edema for OCT).
5. MASTER CODING FOR COMBINED CASES
Surgeons must take specific steps when combining retina and anterior segment procedures (eg, PPV and a repositioning or exchange of an IOL).6 This includes a review of the CPT code descriptor, NCCI edits, and any additional modifiers necessary.
Let’s look at a case study with the following details: an operative report documents a PPV, removal of a dislocated IOL, and insertion of a new IOL, right eye. This procedure is performed outside any global periods. There are several CPT code considerations (Table 3).
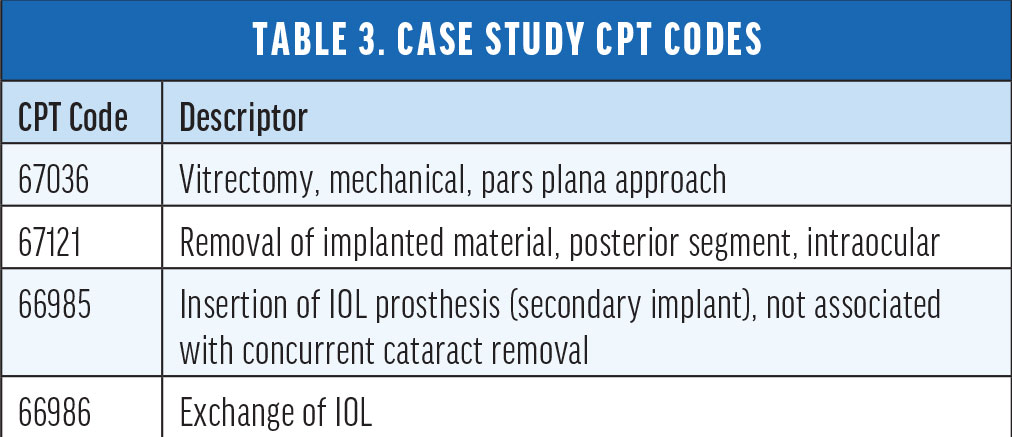
A common error is to code as 67036, 67121, 66985. However, 67036 and 67121 are bundled, and it is not appropriate to unbundle with modifier –59. Moreover, 66985 represents just the secondary implant, and if billed with 67036, does not represent the entire procedure.
The correct coding is 66986–RT and 67036–RT. The order in which you report the codes is crucial; list from highest to lowest RVU so that the multiple procedure reduction (50%) is applied to the second procedure. These two codes are not bundled and appropriately report the surgery performed.
To continue to master the complex world of retina coding, visit aao.org/retinapm and review the 2023 Retina Coding: Complete Reference Guide.
1. Woodke J. Three questions when coding laser therapy. Retina Today. 2022;17(7):54-55.
2. Woodke J. Properly coding retina surgeries. Retina Today. 2019;14(5):54-56.
3. Local coverage determination policies. American Academy of Ophthalmology. Accessed July 26, 2023. www.aao.org/practice-management/coding/lcd-policies/carrier-list
4. Woodke J. Vital Information to Know About Testing Services. Retina Today Business Matters. 2019;1(4):4, 6, 18.
5. 2023 Retina Coding: Complete Reference Guide Book. American Academy of Ophthalmology. 2023. Accessed July 26, 2023. store.aao.org/2023-retina-coding-complete-reference-guide-book.html
6. Woodke J. When multiple procedures are performed in the same session. Retina Today Business Matters. 2021;4(1):2-4.






