


Choroidal folds are undulations in the Bruch membrane located under the retina, often accompanied by retinal pigment epithelium (RPE) and inner choroidal undulations, which can be a sign of ocular or extraocular abnormalities. These findings can occur unilaterally or bilaterally and can present with or without symptoms.1 Choroidal folds appear as hyper- and hypofluorescent lines on fluorescein angiography but can also be visualized on autofluorescent photography as hyper- and hypoautofluorescent linear folds.2
The underlying cause of choroidal folds can be challenging to determine. A thorough evaluation is necessary to tailor management strategies for treatable conditions. In this article, we report a case of unilateral choroidal folds in an adult that were found to be secondary to a rare condition. We also discuss useful diagnostic tests and suggest potential therapies.
CASE REPORT
A 64-year-old White woman was referred to our center following an 8-year history of a bulging left eye that was initially attributed to thyroid eye disease from underlying hypothyroidism. The patient did not have any other ophthalmic or systemic complaints. VA was 20/40 OD and 20/30 OS. IOP and color vision were normal in each eye. Refraction was +4.50 D OD and +6.00 D OS.
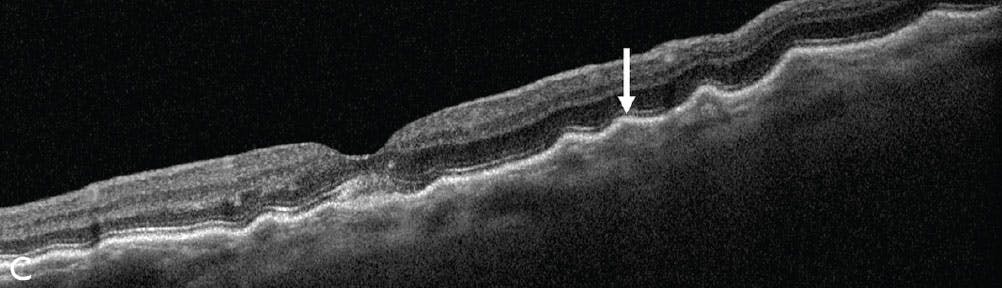
On fundoscopy, horizontal choroidal folds were discovered throughout the macula in the left eye. On wide-angle fundus imaging, the folds were oriented horizontally, which was confirmed on fundus autofluorescence (Figure 1). The vertical section on OCT demonstrated distinct choroidal folds at the level of the choroid and RPE (Figure 2). MRI of the left orbit and left side of the brain revealed a cystic mass in the lacrimal gland fossa (Figure 3A), suggestive of an orbital dermoid cyst with an intraosseous component superotemporally compressing the left globe and giving rise to the choroidal folds (Figure 3B).
Observation, rather than surgical resection with serial imaging, was advised because the patient was asymptomatic.

Figure 1. Fundus photography shows horizontal choroidal folds through the macula (A, arrow). Fundus autofluorescence provides another view of the choroidal folds with alternating hyper- and hypoautofluorescence (B, arrow).
POSSIBLE CAUSES
Choroidal folds are rare and occur at the level of Bruch membrane/choriocapillaris, appearing as organized parallel lines with globe compression, circumferential lines in the juxtapapillary region with optic disc elevation, or randomly oriented lines, in the case of hypotony.
Jaworski et al proposed four distinct causes for the formation of choroidal folds: deformation of the sclera due to optic nerve traction, thickening or shrinkage of the sclera, decreased scleral rigidity, and contraction of the sub-RPE in neovascularization.4 On ophthalmoscopy, choroidal folds appear as alternating bright and dark parallel streaks or lines that vary in length and width, typically in the post-equatorial region and predominantly involving the macular region. The less-pigmented lines correspond to RPE thinning, while the darkly pigmented intervening lines represent RPE compression.5

Figure 3. Axial view MRI (T1 weighted, no fat suppression) reveals an orbital dermoid cyst superotemporally (A, arrow) with globe compression. Coronal view MRI (T2 weighted) shows the dermoid cyst with an intraosseous component (B, arrow).
ASSOCIATED CONDITIONS
Choroidal folds can be associated with several ocular and extraocular pathological conditions. In a retrospective comparison study of unilateral versus bilateral chorioretinal folds, Leahey et al found that unilateral folds were due to scleritis (17%), hypotony (13%), vascular occlusion (13%), intraocular tumors (13%), AMD (10%), optic nerve edema (7%), retinal detachment (7%), hyperopia (3%), orbital tumor (3%), trauma (3%), optic atrophy (3%), and orbital bone compression (3%).5 Furthermore, they found that bilateral folds were due to AMD (29%), hyperopia (25%), idiopathic (21%), hypotony (8%), scleritis (4%), thyroid eye disease (4%), uveitis (4%), and choroiditis (4%).5
Diagnosis and characterization of choroidal folds often requires functional analysis of the eye, tonometry, and imaging, such as color fundus photography, fluorescein angiography, ICG angiography, autofluorescence, OCT, and ultrasonography.3,5 Currently, OCT is the most specific tool to enable differentiation of choroidal folds from retinal folds secondary to other causes, such as epiretinal membrane and complications post-retinal detachment surgery.1,6
In this case, MRI was key to establishing the cause of the choroidal folds with the delineation of an orbital dermoid cyst with globe compression. Orbital dermoid cyst is traditionally a childhood cystic tumor, often requiring surgical removal. In a retrospective study of 197 consecutive orbital and periorbital dermoid cysts from an ocular pathology laboratory over a 32-year period, Shields et al found that the mean age at surgical excision was 17 years; moreover, only 9% of the cysts were first diagnosed in patients 50 years of age and older, with the oldest patient being 85 years of age.7 A dermoid cyst can originate superotemporally (72%), superonasally (17%), or in other locations (11%) within the orbit. Orbital dermoid cysts are classically managed with surgical excision, cyst aspiration and sclerotherapy, or observation.8
Our decision to follow the patient with serial imaging (OCT) was based on the chronic and asymptomatic nature of her disease.
FIND THE ROOT CAUSE
Choroidal folds are an important clinical sign that suggests the presence of a possible underlying ocular or orbital disease. The evaluation of the cause of choroidal folds should include taking a detailed medical history, clinical assessment, and imaging. Treatment should be individualized for each patient, depending on the underlying pathology.
Support provided in part by the Eye Tumor Research Foundation, Philadelphia, PA (CLS). The funders had no role in the design and conduct of the study, in the collection, analysis and interpretation of the data, and in the preparation, review or approval of the manuscript. Carol L. Shields, MD, has had full access to all the data in the study and takes responsibility for the integrity of the data.
1. Grosso D, Borrelli E, Sacconi R, Bandello F, Querques G. Recognition, diagnosis and treatment of chorioretinal folds: current perspectives. Clin Ophthalmol. 2020;14:3403-3409.
2. Cangemi FE, Trempe CL, Walsh JB. Choroidal folds. Am J Ophthalmol. 1978;86(3):380-387.
3. Newell FW. Choroidal folds. The seventh Harry Searls Gradle Memorial lecture. Am J Ophthalmol. 1973;75(6):930-942.
4. Jaworski A, Wolffsohn JS, Napper GA. Aetiology and management of choroidal folds. Clin Exp Optom. 1999;82(5):169-176.
5. Leahey AB, Brucker AJ, Wyszynski RE, Shaman P. Chorioretinal folds. A comparison of unilateral and bilateral cases. Arch Ophthalmol. 1993;111(3):357-359.
6. Heimann H, Bopp S. Retinal folds following retinal detachment surgery. Ophthalmologica. 2011;226(Suppl 1):18-26.
7. Shields JA, Kaden IH, Eagle RC, Jr, Shields CL. Orbital dermoid cysts: clinicopathologic correlations, classification, and management. The 1997 Josephine E. Schueler Lecture. Ophthalmic Plast Reconstr Surg. 1997;13(4):265-276.
8. Bagnis A, Cutolo CA, Corallo G, Musetti D, Nicolo M, Traverso CE. Chorioretinal folds: a proposed diagnostic algorithm. Int Ophthalmol. 2019;39(11):2667-2673.










_1773249222.png?auto=compress,format&w=75)








