


AT A GLANCE
- Peeling the internal limiting membrane and epiretinal membranes has become the standard technique to address vitreomacular interface diseases.
- Human amniotic membrane transplant and autologous retinal transplant are recent approaches to the treatment of refractory macular holes.
- Retinal expansion is a valuable technique for macular holes, in which subretinal injection of balanced salt solution creates a macular detachment.
The assessment of the vitreomacular interface has evolved significantly, and we can now accurately determine its histological architecture like never before. OCT and OCT angiography are the most relevant tools available to help clinicians image and evaluate changes in the posterior pole. These imaging capabilities have given rise to improved macular surgery performance and better communication with the patient about their condition, both of which have improved care.
CONDITIONS WE TREAT
Epiretinal membranes (ERMs), vitreomacular traction, and full-thickness macular holes (FTMHs) are the most common disorders that can arise due to vitreoretinal interface changes. Currently, these conditions are treated with surgery.
ERMs and Vitreomacular Traction
In the past, ERMs were considered an epiretinal phenomenon caused by two vectors of traction: anteroposterior and tangential. This is now known as vitreomacular traction syndrome (VMTS), where 20% of the population is asymptomatic; some patients may experience spontaneous resolution, while others progress to a FTMH.1-3
In 2016, the PACORES group published a retrospective multicenter study of 168 eyes, of which 21.4% (36 eyes) showed spontaneous resolution of VMTS after a mean follow-up of 11.4 ± 12.6 months. An unfavorable anatomic outcome occurred in 7.7% (13 eyes). In addition, the study found that the baseline spectral-domain OCT grade may predict the progression to FTMH.4
In 2017, Govetto et al published a new OCT staging scheme for ERMs, in which ERMs were classified based on foveal thickness measures and the identification of specific biomarkers, such as the presence of ectopic inner foveal layers. The ability to properly classify ERMs is crucial to achieve optimal results in our everyday practice.5
The OCT-based staging scheme uses morphologic and functional characteristics to classify ERMs into four stages: presence of the foveal pit and well-defined retinal layers (stage 1); absence of the foveal pit and well-defined retinal layers (stage 2); absence of the foveal pit, well-defined retinal layers, and presence of ectopic inner foveal layers (stage 3); and absence of the foveal pit, disrupted retinal layers, and presence of ectopic inner foveal layers (stage 4).5
This classification is clinically relevant and has prognostic implications because higher stages correlate with worse visual acuity outcomes.
Macular Holes
To determine the appropriate treatment approach for FTMHs, we first measure the hole size and the baseline visual acuity. Based on these criteria, clinicians can decide to monitor, treat medically, or proceed to the OR. A surgical approach to FTMHs has three main objectives: lower the resistance to facilitate the closure with the maculorexis; decrease the size by drying with fluid-air exchange; and provide a gas tamponade (SF6).6
One of the most disruptive innovations in the field was made in 1997 by C. Eckardt, who published the results of macular holes that were treated with vitrectomy plus internal limiting membrane (ILM) peeling (Figure 1A).7 The procedure—novel at the time—led to an unprecedented 92% success rate, ushering in an era of ILM peeling as the standard for FTMHs.7
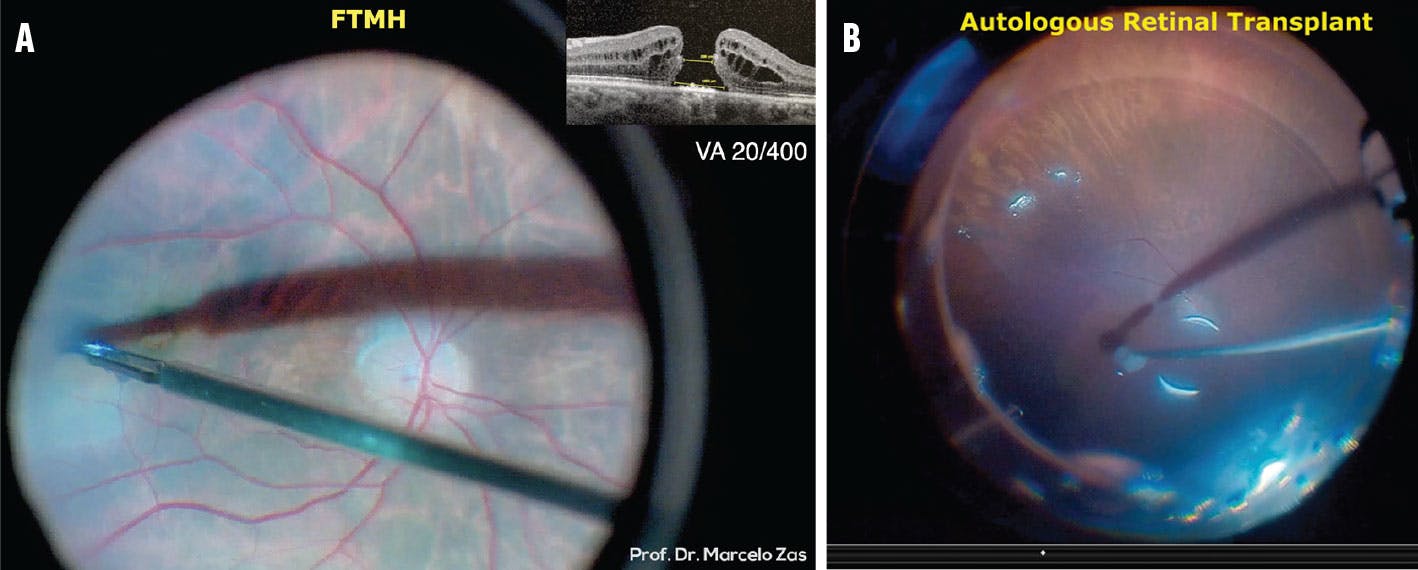
Figure 1. ILM peeling (A) became a standard surgical approach to FTMHs after C. Eckardt published on the technique in 1997. ART (B) may be a useful technique for refractory macular holes, leading to good anatomic and functional outcomes.
A few years later, Michalewska et al described the inverted ILM flap technique, which improved both functional and anatomic outcomes of vitrectomy for FTMHs with a diameter greater than 400 µm.8
More recently, Wiedemann provided insight into the mechanisms of ILM peeling, including improved retinal flexibility, better oxygen supply to the inner retina, and, potentially, retinal glial cell proliferation. These mechanisms lead to reduced foveal thickness and improved visual acuity, closure rates, and macular function.9
Despite this growing body of work, we have yet to find a definitive solution for macular holes. Many FTMHs that are refractory to conventional management may be less than 400 µm, requiring a revised classification scheme and novel treatment options.10 At the 2019 Retina World Congress, Tamer H. Mahmoud, MD, PhD, presented on autologous retinal transplantation (ART) for macular holes, adding to our growing armamentarium. Human amniotic membrane transplant (hAM) is yet another recent technique that has made the treatment of recurrent and refractory FTMHs possible.11,12 Both are equally valid and widely accepted.
With the capability to enhance epithelial cell growth, hAM is a well-known adjuvant used for the treatment of corneal and conjunctival defects. The initial technique, described by Rizzo et al, used bimanual manipulation to insert the graft into the subretinal space under perfluorocarbon liquid.11 The restoration of the retinal layers observed in the postoperative period resembles a healthy eye, suggesting that the amniotic cells are inducing tissue remodeling.11
A large retrospective case series of 130 patients undergoing ART for the repair of primary and refractory macular holes showed good anatomic and functional outcomes (Figure 1B). In the study, 89% of macular holes closed (78.5% complete; 10% small eccentric defect), visual acuity improved by at least 3 lines in 43% of eyes and at least 5 lines in 29% of eyes, and there were low complication rates.12
Several alternative surgical options may prove useful for certain refractory macular holes, such as various ILM flap techniques, retinal expansion, lens capsule transplantation, blood products, and macular buckling.
The CLOSE study group examined a total of 1,135 eyes and proposed a surgical classification for large FTMHs based on surgical techniques. The study found that large (400 µm – 550 µm) and X-large (550 µm – 800 µm) holes can be successfully treated with ILM peeling and ILM flap techniques, respectively. The team noted that further studies are necessary for XX-large (≥ 800 µm – < 1,000 µm) and giant macular holes (≥ 1,000 µm) to determine which technique is best based on hole size and characteristics.13
Parolini et al published a classification and management system for patients with myopic traction maculopathy (MTM), which suggests that surgeons should observe early stages of MTM but address schisis and detachments with macular buckling. FTMHs should be treated with vitrectomy and ILM peeling to alleviate the tangential forces.14
The retinal expansion technique is another valuable alternative to macular hole closure. Subretinal injection of balanced salt solution creates a macular detachment, which may lead to hole closure. Our team recently published a retrospective interventional case series of two patients with chronic FTMHs who were treated with retinal expansion; one patient achieved complete hole closure.15
Alezzandrini et al published a study to compare the functional and anatomic outcomes at 24 months of eyes with a primary FTMH that failed to close after surgery and were treated with either an ART of ILM (ART-ILM) or the retinal expansion technique (Figure 2). Patients in the ART-ILM group (n = 14) experienced a statistically significantly improved BCVA (median 49.5, range 20–66 letters) compared with preoperative BCVA (median 39 letters). In contrast, patients in the retinal expansion group (n = 14) did not achieve a statistically significant improvement. At 24 months, 85.7% of patients in the ART-ILM group achieved closure compared with 57.1% in the retinal expansion group (Tables 1 and 2). The baseline macular hole size was not a significant preoperative factor that influenced closure rates.16
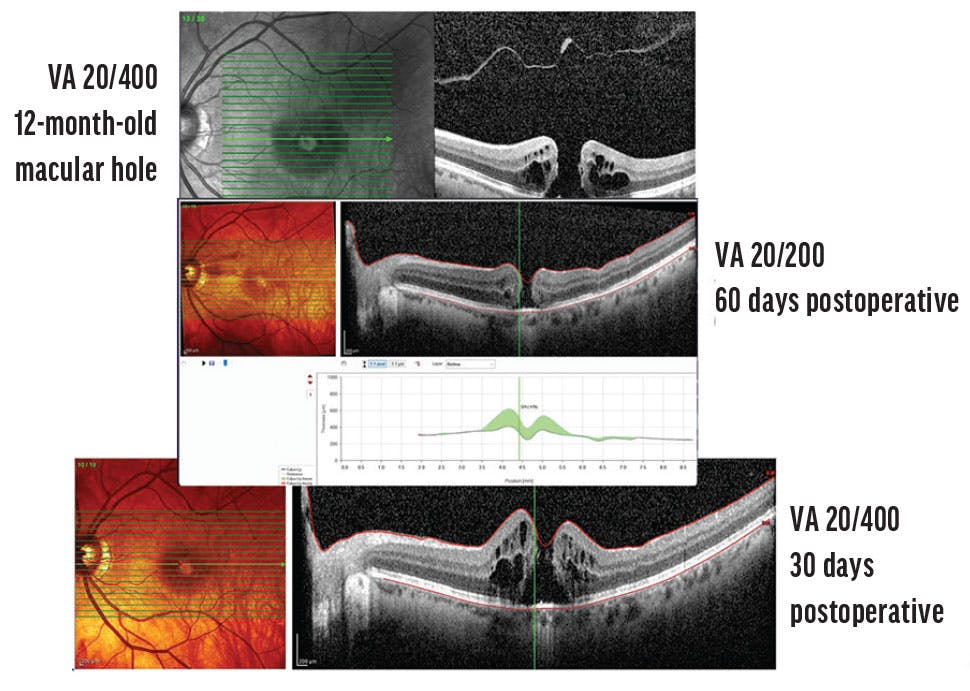
Figure 2. Although retinal expansion may help to close refractory FTMHs, recent research suggests patients may not experience significantly improved vision postoperatively.


NOVEL TECHNIQUES ON THE RISE
Macular surgery has been a hot topic in retina for years, fostering the growth of many novel techniques. With advanced diagnostics and imaging, we now embrace the fact that functional results are as equally relevant as anatomic outcomes. Thus, we must begin assessing the visual function of our patients using BCVA, microperimetry, mERG, and multimodal images. These postoperative evaluations could provide surgeons with significant insight into the true nature of our surgical results.
1. Hikichi T, Yoshida A, Trempe CL. Course of vitreomacular traction syndrome. Am J Ophthalmol. 1995;119(1):55-61.
2. Girach A, Pakola S. Vitreomacular interface diseases: pathophysiology, diagnosis and future treatment options. Expert Rev Ophthalmol. 2012;7(4);311-323.
3. Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120(12):2611-2619.
4. Wu L, Zas M, Berrocal MH, et al. Anatomical and functional outcomes of symptomatic idiopathic vitreomacular traction: A Natural History Study from the Pan American Collaborative Retina Study Group. Retina. 2016;36(10):1913-1918.
5. Govetto A, Lalane RA 3rd, Sarraf D, Figueroa MS, Hubschman JP. Insights into epiretinal membranes: presence of ectopic inner foveal layers and a new optical coherence tomography staging scheme. Am J Ophthalmol. 2017;175:99-113.
6. Zhao P, Wang S, Liu N, Shu Z, Zhao J. A review of surgical outcomes and advances for macular holes. J Ophthalmol. 2018;2018:7389412.
7. Eckardt C, Eckardt U, Groos S, et al. Removal of the internal limiting membrane in macular holes. Clinical and morphological findings. Ophthalmologe. 1997;94:545-551.
8. Michalewska Z, Michalewski J, Adelman RA, et al. Inverted internal limiting membrane flap technique for large macular holes. Ophthalmology. 2010;117(10):2018-2025.
9. Wiedemann P. How internal limiting membrane peeling revolutionized macular surgery in the last three decades. Int J Ophthalmol. 2023;16(6):837-840.
10. Marlow ED, Mahmoud TH. Current management strategies for atypical macular holes. Taiwan J Ophthalmol. 2020;11(3):221-231.
11. Rizzo S, Caporossi T, Tartaro R, et al. A human amniotic membrane plug to promote retinal breaks repair and recurrent macular hole closure. Retina. 2019;39(Suppl 1):S95‐103.
12. Moysidis SN, Koulisis N, Adrean SD, et al. Autologous retinal transplantation for primary and refractory macular holes and macular hole retinal detachments: The Global Consortium. Ophthalmology. 2021;128(5):672-685.
13. Rezende FA, Ferreira BG, Rampakakis E, et al. Surgical classification for large macular hole: based on different surgical techniques results: the CLOSE study group. Int J Retin Vitreous. 2023;9(1):4.
14. Parolini B, Palmieri M, Finzi A, Besozzi G, Frisina R. Myopic traction maculopathy: a new perspective on classification and management. Asia Pac J Ophthalmol. 2021;10(1):49-59.
15. Zas M, Lasave AF, Alfano A, Saravia M. Surgical technique for approaching chronic or persistent macular holes: two case reports. Am J Ophthalmol Case Rep. 2020;18:100692.
16. Alezzandrini A, Dorrego CI, Cibrán MV, et al. A 24-month follow-up of refractory macular holes treated with an autologous transplantation of internal limiting membrane versus retina expansion technique. Int J Retina Vitreous. 2021;7(1):57.






_1784132761.jpg?auto=compress,format&w=75)











