
Reviewed by Cindy X. Cai, MD
AT A GLANCE
- Lapses in care for patients with diabetic retinopathy (DR) range from 10% to 61%.
- Patients who are Black, Hispanic, and other race/ethnicity who live in more socioeconomically disadvantaged neighborhoods are more likely to have lapses in care compared with non-Hispanic White patients in more advantaged neighborhoods.
- Where a patient lives can have a significant effect on their ability to seek screening for diabetic eye disease and adhere to ongoing DR care.
With proliferative diabetic retinopathy (PDR) standing as the leading cause of vision loss in patients with diabetes,1,2 retina specialists are keenly aware that lapses in care for this patient population can lead to lower BCVA and increased rates of vitrectomy.3
However, one study of 418 patients with PDR undergoing anti-VEGF injections or panretinal photocoagulation therapy found that 61% were lost to follow-up (LTFU) at 4 years.4 Another larger study of 4,423 patients with PDR found that 54.4% and 52.4% were completely LTFU at 6 months and 1 year, respectively.5 Other studies have reported more modest rates of 10% to 16%.3,6
Given the potentially devastating visual consequences of lapses in care,7 researchers continue to explore the risk factors and patient-specific causes for such lapses that might be addressed in the clinic to improve the patient’s chances of adhering to treatment and preserving their vision. For example, Khurana et al found that Black or African American race/ethnicity, Hispanic ethnicity, baseline vision worse than 20/40, having private insurance, living in the South, and unilateral disease were all risk factors for LTFU.6
Recently, researchers have dug further to uncover the link between where a person lives and lapses in their DR care.
APPLYING SOCIAL DETERMINANTS OF HEALTH TO DR CARE
A team at the Wilmer Eye Institute at Johns Hopkins School of Medicine completed a retrospective cohort study of 36,497 adult patients with diabetes who were seen at the clinic for DR screening or treatment.8
Using the electronic health record, the team identified each patient’s level of neighborhood socioeconomic disadvantage, measured by the 2019 area deprivation index (ADI) and divided into quartiles, with Q4 indicating the most socioeconomic disadvantage (Figure).9 Of the patients included in the study, 13,335 were in ADI Q1; 12,330 were in Q2; 6,025 were in Q3; and 4,511 were in Q4. Other demographic data included in the analysis were race and ethnicity, the distance patients lived from the clinic, DR severity, and the diagnosis of other retinal/ocular disorders.
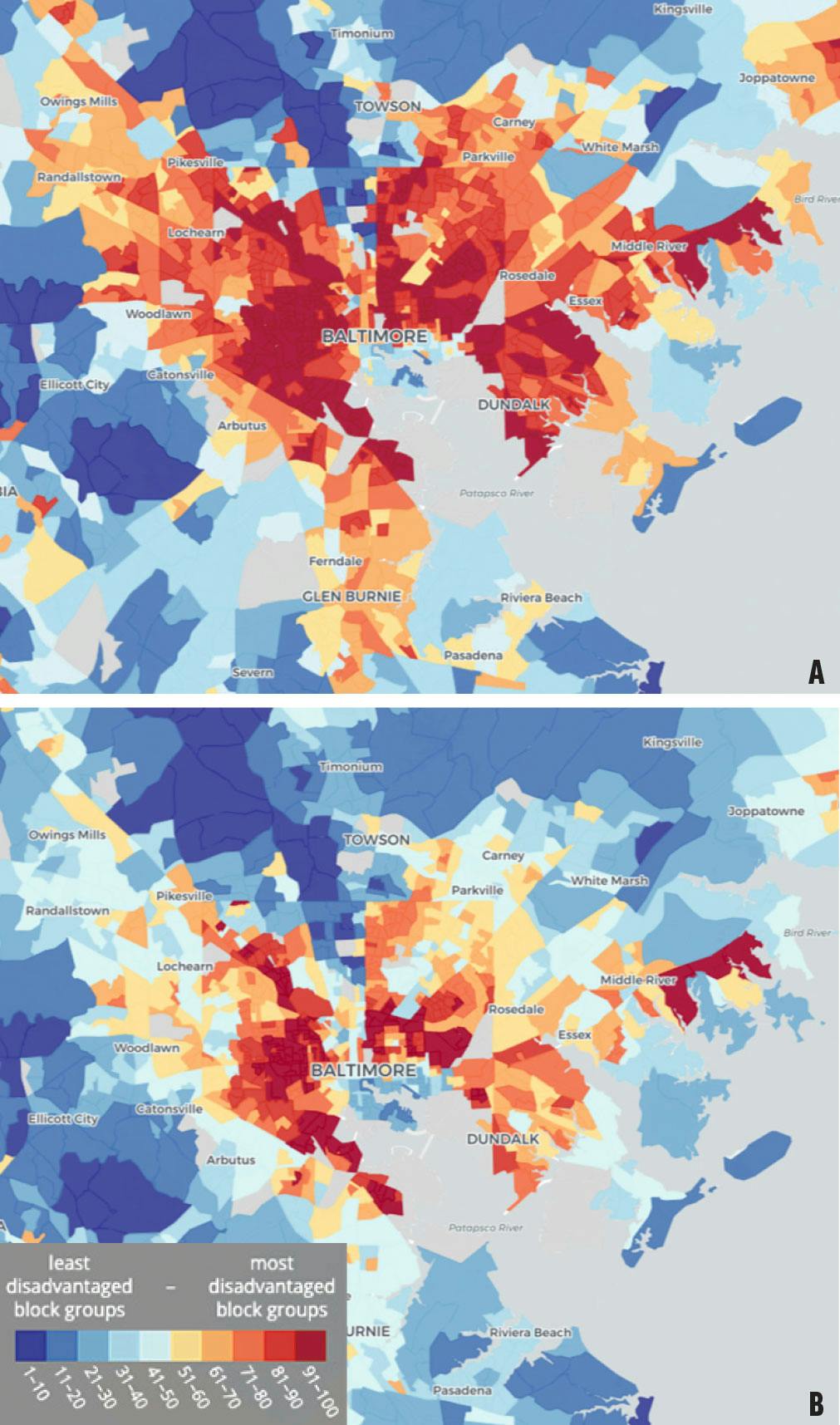
Figure. The ADI for the Baltimore area shows the socioeconomic conditions of each neighborhood, as compared with state-wide (A) and national (B) scores.9
ABOUT THE AREA DEPRIVATION INDEX
The Area Deprivation Index, created by researchers at the University of Wisconsin School of Medicine and Public Health, uses public data on income, education, employment, and housing to rank neighborhoods compared with the country and the state. Visit The Neighborhood Atlas to learn more.
Study Findings
Of the patients included, 63% had a lapse in DR care (defined as a deviation from the provider’s recommended follow-up timeframe) over 2 years. When broken down based on ADI, 60% of patients in ADI Q1 were LTFU (at least intermittently), 62% in Q2, 66% in Q3, and 68% in Q4.8
In addition, there was a statistically significant interaction between ADI and race and ethnicity (P = .005). For example, non-Hispanic White patients from more disadvantaged neighborhoods (ie, ADI Q4) had higher odds of lapses in care compared with those in Q1 (odds ratio [OR] of 1.68). Pairwise comparisons revealed that patients who were Black, Hispanic, and other race/ethnicity who were in higher ADI quartiles had higher odds of LTFU compared with non-Hispanic White patients in Q1 and Q2. For example, patients with other race/ethnicity in Q4 were nearly twice as likely to have lapses in care (OR = 1.88) compared with non-Hispanic White patients in Q1. Compared with non-Hispanic White patients in Q1, Black patients in Q4 had an OR of a lapse in care of 1.36. Of note, Black patients in more socioeconomically advantaged neighborhoods were less likely to experience lapses in care compared with their counterparts in more disadvantaged neighborhoods.8
ABOUT THE SPEAKERS

Cindy X. Cai, MD
• Jonathan and Marcia Javitt Rising Professor of Ophthalmology, Wilmer Eye Institute, Johns Hopkins School of Medicine, Baltimore
WHY IT MATTERS
The data presented here reinforce the role neighborhood-level social determinants of health play in DR care. Patients with diabetes who live in more socioeconomically disadvantaged neighborhoods (eg, who might have limited access to public transportation), regardless of their race and ethnicity, have a higher odds of experiencing lapses in care. Still, race and ethnicity remain crucial factors, given that patients who identify as any race/ethnicity other than non-Hispanic White from nearly all neighborhoods were more likely to be LTFU compared with non-Hispanic White patients in the lower ADI quartiles. The study also revealed that living in a more advantaged neighborhood may help to reduce the adverse effects of structural racism on the use of eye care among Black patients with diabetes.
While more research is necessary to better understand the relationships between individual, community, and societal factors and DR care, it is clear that where a patient lives can have a significant effect on their ability to seek screening for diabetic eye disease and adhere to ongoing DR care.
However busy we are in our clinics, we must not lose sight of these patient-level factors and work together with our patients and local communities to ensure everyone receives the care they need to preserve their vision.
1. Aiello LP. Angiogenic pathways in diabetic retinopathy. N Engl J Med. 2005;353(8):839-841.
2. Antonetti DA, Klein R, Gardner TW. Diabetic retinopathy. N Engl J Med. 2012;366(13):1227-1239.
3. Abdelmotaal H, Ibrahim W, Sharaf M, Abdelazeem K. Causes and clinical impact of loss to follow-up in patients with proliferative diabetic retinopathy. J Ophthalmol. 2020;2020:7691724.
4. Green M, Tien T, Ness S. Predictors of lost to follow-up in patients being treated for proliferative diabetic retinopathy. Am J Ophthalmol. 2020;216:18-27.
5. Suresh R, Yu HJ, Thoveson A, et al. Loss to follow-up among patients with proliferative diabetic retinopathy in clinical practice. Am J Ophthalmol. 2020;215:66-71.
6. Khurana RN, Wang JC, Zhang S, Li C, Lum F. Loss to follow up in patients with proliferative diabetic retinopathy treated with anti-VEGF therapy and/or panretinal photocoagulation in the United States [published online ahead of print April 23, 2024]. Ophthalmol Retina.
7. Obeid A, Su D, Patel SN, et al. Outcomes of eyes lost to follow-up with proliferative diabetic retinopathy that received panretinal photocoagulation versus intravitreal anti-vascular endothelial growth factor. Ophthalmology. 2019;126(3):407-413.
8. Tang T, Tran D, Han D, Zeger SL, Crews DC, Cai CX. Place, race, and lapses in diabetic retinopathy care. JAMA Ophthalmol. 2024;142(6):581-583.
9. Neighborhood Atlas. Center for Health Disparities Research. University of Wisconsin School of Medicine and Public Health. Accessed June 6, 2024. www.neighborhoodatlas.medicine.wisc.edu




_1784132761.jpg?auto=compress,format&w=75)











