
AT A GLANCE
- In the pivotal trial, 96.1% of patients successfully used the home OCT device that was shipped to them with no or only virtual support.
- After reviewing home OCT data, physicians would not have treated 42% of patients who were treated in the real world.
- There is a dedicated code, 0606T, set for the reimbursement of work performed by the prescribing physician, or other qualified health care professional, to review home OCT data.
Remote and home monitoring is prevalent in endocrinology and cardiology in the form of continuous glucose monitors and electrocardiogram wearables. The experiences in those domains can be helpful for retina practices as we adopt digital tools such as the Scanly Home OCT (Notal Vision). In this article, I discuss how home OCT can be incorporated into clinical care for maximum benefit to the patient.
THE PROCESS
To initiate home OCT, the retina specialist sends a prescription to the monitoring service center responsible for administering the program. The system does not require a clinic to carry the device, train the patient, or help with logistics such as device setup and insurance verifications—these details are managed by a dedicated monitoring center. In the pivotal trial, 96.1% of patients successfully used the home OCT device that was shipped to them with no or only virtual support.1
Once a patient starts using the home OCT system, physicians receive automated, HIPAA-compliant notifications of the data to review. The notifications are generated based on physician-set parameters related to anatomic changes or time elapsed since the last review.
The anatomic features that are identified on home OCT are hyporeflective spaces, which are abnormal dark areas in the retinal space that are often, but not always, indicative of retinal fluid.
A second pivotal trial investigated and validated the performance of an AI-based system, the Notal OCT Analyzer, that automatically segments hyporeflective spaces and estimates the volume.2
The home OCT data is reviewed in a dedicated portal that has both OCT scans and quantitative estimates from the AI algorithm that helps the retina specialist determine the need for an office visit(Figure).
There is a dedicated code, 0606T, set for the reimbursement of work performed by the prescribing physician, or other qualified health care professional, to review the home OCT data. The code can be billed once every 30 days.
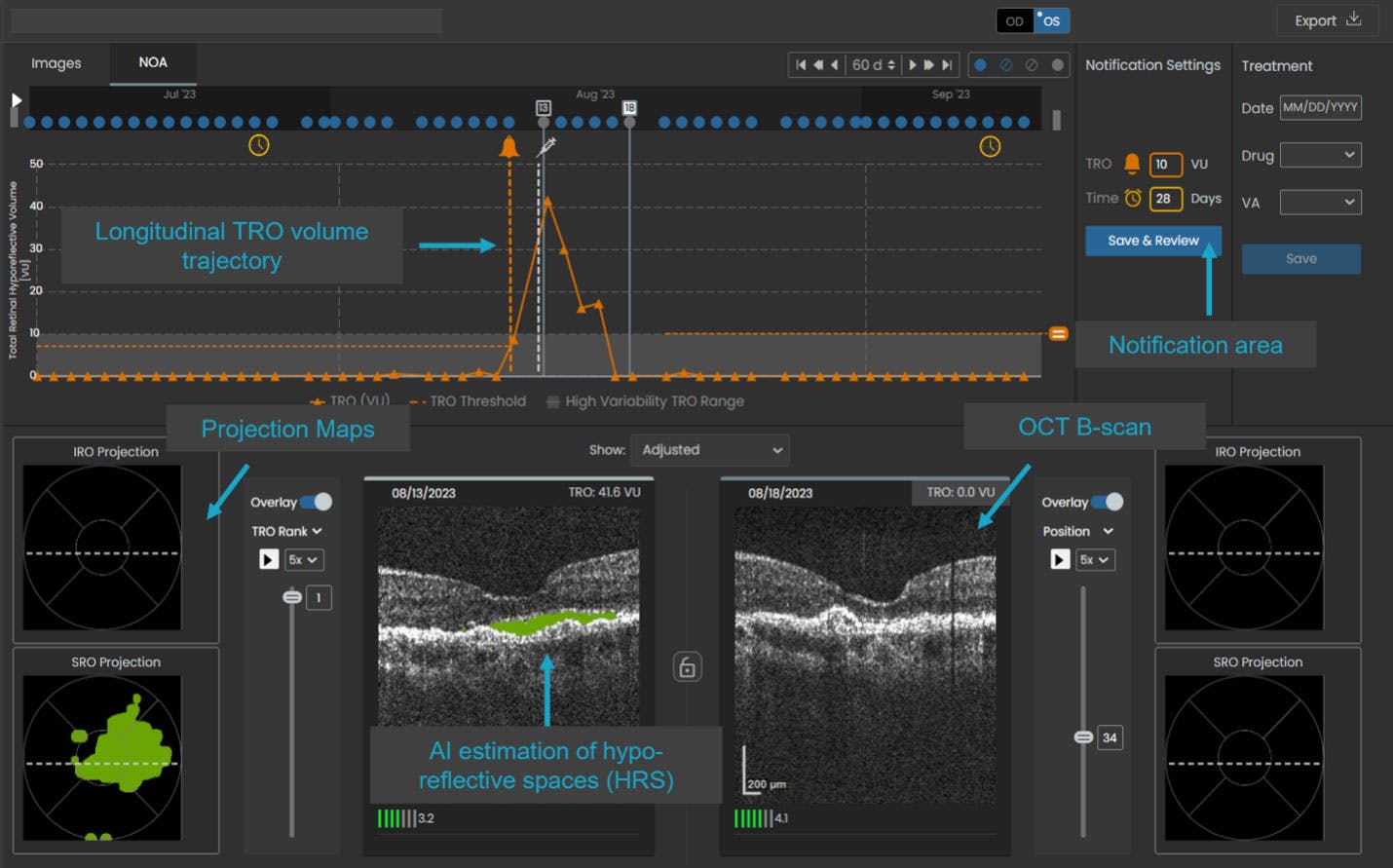
Figure. The SCANLY portal provides raw OCT scans for review and AI-generated parameters for additional insights. Physicians can set appropriate parameters to receive notifications that prompt a review.
PATIENT CARE
Two studies have assessed the effect of home OCT on patient care. A prospective trial showed that the number of treatments dropped, on average, when wet AMD patients switched from standard-of-care treat-and-extend management to home OCT-based management.3 At the same time, some patients were treated more frequently due to early detection of disease activity.3 Another study looked at how home OCT data affected physician decision making. After reviewing home OCT data, physicians would not have treated 42% of patients who were treated in the real world.4 In addition, when the physicians did make the decision to treat based on home OCT data, in more than 60% of cases they would have treated the patients at least a week earlier compared with actual care.4
PERSONAL EXPERIENCE
Based on study data and my own personal experience with the system, I believe home OCT will be useful for patients in different stages of wet AMD management in unique ways. In the early stages of disease management, the device may help us better understand what treatments are most effective for a given patient. This becomes possible because home OCT provides highly granular temporal data, giving us unprecedented insight into the treatment response. The variability of the response to treatment in early stages of the disease was well demonstrated by DRCR Retina Network’s Protocol AK.5
Once the patient has an established treatment regimen, home OCT may help clinicians pinpoint the optimal treatment interval without having to extend patients in steps of 1 to 2 weeks, potentially reducing the burden on patients and caregivers and the risk of treatment dropout. Patients on longer extensions can have the safety net of home OCT to catch a sudden recurrence of disease activity that can often lead to significant vision loss.
Finally, for patients who reach a stable stage with no signs of disease activity for extended periods, home OCT can allow for monitoring with monthly or AI-prompted reviews by the physician.
Patients who are particularly anxious about their disease or find it difficult to make office visits may be good candidates for a remote monitoring service, although clinicians must be aware of possible comorbidities that prevent patients from using the device.
For more on remote monitoring in cardiology, check out this feature in Retina Today:
Adopting Remote Monitoring and AI: Lessons From Cardiology
By Judy E. Kim, MD, FARVO, FASRS, and Jagmeet P. Singh, MD, ScM, PhD, FHRS, FACC
IMPACT ON RETINA PRACTICES
The adoption of any new management paradigm is always a challenge for busy retina clinics. Like any new digital tool, it comes with a learning curve, and clinicians will have to integrate the review of notifications and learn how to schedule patients based on those reviews. Staff participation will be key in the execution and success of remote digital technology.
A practical component related to the adoption of home OCT will be reimbursement associated with the data review. The dedicated reimbursement code creates a new potential revenue stream for participating clinics.
An objective source of information, and potential best practices, can come from other domains of medicine where remote monitoring is widely used. The strong adoption of remote cardiac monitoring and the prevalence of continuous glucose monitoring show that such digital tools can become a net benefit to the providers. In addition, when a new category 1 code is covered by the Centers for Medicare and Medicaid Services, budget neutrality is applied across codes from all specialties, not just for the specialty that is introducing a new code. Thus, specialties introducing innovation are set to benefit from the effort that goes behind it.
There has never been a better time to be part of innovations poised to benefit patients, providers, and the health care system. The adoption of home-based monitoring may be a foundational step toward the era of digital medicine in retinal disease management.
1. Home OCT fluid visualization agreement study. Assessed March 3, 2025. clinicaltrials.gov/study/NCT04907409
2. Schneider EW, Heier JS, Holekamp NM, et al. Pivotal trial toward effectiveness of self-administered OCT in neovascular age-related macular degeneration. Report 2-artificial intelligence analytics. Ophthalmol Sci. 2024;5(2):100662.
3. Holekamp NM, Beus A, Clark WL, Heier JS. Prospective study of home OCT guided management of treatment experience nAMD patients. Retina. 2024;44(10):1714-1731.
4. Heier JS, Liu Y, Holekamp NM, et al. Clinical use of home OCT data to manage neovascular age-related macular degeneration. J Vitreoretin Dis. 2024:24741264241302858.
5. Blinder, Calhoun C, Maguire MG, et al. Home OCT imaging for newly diagnosed neovascular age-related macular degeneration: a feasibility study. Ophthalmol Retina. 2024;8(4):376-387.


_1784132761.jpg?auto=compress,format&w=75)











