


AT A GLANCE
- Based on data from the Primary Retinal Detachment Outcomes Study, patients 80 years and older were more likely to present with macula-off detachments and preoperative proliferative vitreoretinopathy compared with patients 40 to 79 years old.
- Rhegmatogenous retinal detachment surgery was often more complex in elderly patients and more likely to require membrane peeling, intraoperative perfluoro-n-octane, and silicone oil tamponade.
- Postoperative positioning is crucial to ensure a successful retinal detachment repair; however, postoperative positioning may not be possible for some older adults because of concomitant musculoskeletal disorders.
- In elderly patients, the mean VA improved from preoperative 20/500 to postoperative 20/125, compared with 20/200 to 20/40 in younger patients.
As you walk through the clinic of a vitreoretinal specialist, you often find a disproportionate number of older adults in the waiting room. And given that more than 46 million US adults are 65 and older—a number expected to grow to more than 90 million by 2050—this is no surprise.1 According to the AAO’s Committee on Aging, ophthalmologists are second only to geriatricians in the number of patients they see who are older than 65 years.
AMD today accounts for the majority of a vitreoretinal specialist’s work with elderly patients, but other conditions are on the rise as the US population ages, including rhegmatogenous retinal detachment (RRD).1 The prevalence of RRD has a bimodal distribution: a peak at young ages (attributed to high myopia and trauma) and a greater peak between 60 and 69 years.2
But what about elderly patients? Octogenarians and nanogenarians are an increasingly important segment of our society and our clinical practices, yet there is little in the literature describing the presentation and outcomes of older adults with RRD. Many factors can make RRD surgery challenging in the elderly patient. For example, positioning after vitrectomy-based procedures may be difficult for those with cervical and lumbar issues, and following postoperative instructions may be challenging for those with Alzheimer disease and other dementias. Patients in their 80s and 90s also have a higher incidence of hearing impairment, which can lead to difficulties communicating in the OR and during postoperative care. Higher anesthesia risk and medical comorbidities are also important considerations.
To better understand the characteristics and treatment outcomes of RRD in elderly patients, our group analyzed data from the Primary Retinal Detachment Outcomes (PRO) study, a large, comprehensive, observational data set from all patients at six centers who underwent primary RRD repair. Within the PRO database, we compared the presentations and outcomes of those over age 80 who underwent repair of RRD with patients between ages 40 and 79.3
COMPLEX PRESENTATIONS
When compared with younger adult patients (40–79), elderly patients (80 and older) were more likely to present with macula-off retinal detachments (49% vs 66%, respectively, P < .001) and preoperative proliferative vitreoretinopathy (7% vs 13%, respectively, P = .023). Furthermore, 59% of the elderly patients presented with VA worse than 20/200, and the mean presenting VA was much worse for elderly patients (20/500) compared with those in the younger cohort (20/200, P < .001).3
One factor contributing to this disparity may be that elderly patients have poorer access to eye care at multiple levels. For example, a population-based study of 6,775 elderly patients in community dwellings in the Netherlands identified older age (> 85), being homebound due to health reasons, and having lower Mini Mental Status Exam scores as risk factors for untreated cataract.4 Further, in a study in Baltimore, nursing home residents were found to be more than 13 times more likely to be legally blind (VA > 20/200) than community dwelling adults of the same age.5 In that study, 40% of the cases of visual impairment were treatable or preventable, with cataract surgery being the most important factor.
Examining risk factors for preventable and reversible causes of blindness in the elderly provides insight into the delayed and more complex nature of RRD in this population.
COMPLEX REPAIRS
Before undertaking surgery in an elderly patient, surgeons must carefully consider the type of anesthesia they will use. Although general anesthesia poses more risks with increased comorbidities, it may be necessary in certain cases such as for patients with an inability to hold still or maintain the correct positioning or those with physical disability or cognitive difficulties.6,7 In our cohort of patients, most underwent monitored anesthesia care and local anesthesia, and not general anesthesia.3
The majority of elderly patients in our cohort were pseudophakic (90% vs 44% in the younger patients, P < .001), and the most common procedure performed was pars plana vitrectomy (PPV) alone (74%), followed by PPV in combination with a scleral buckle (SB; 27%). However, the surgery itself was often more complex in elderly patients, as the older patients were more likely to require membrane peeling, intraoperative perfluoro-n-octane, and silicone oil tamponade (Figure).
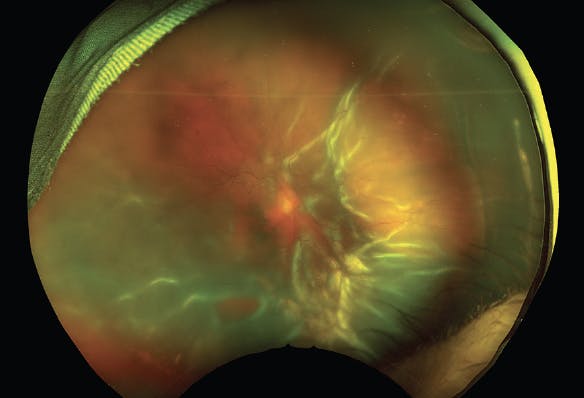
Figure. This is the fundus photograph of an 87-year-old male with multiple medical comorbidities, including newly diagnosed atrial fibrillation. He presented with decreased vision for approximately 2 months during a recent prolonged hospitalization for COVID-19 that required ICU support. On examination, he was pseudophakic with a VA of hand motions. He had a macula-off RRD with star folds and a large inferior break—all suggestive of chronicity. He underwent PPV, membrane peel, inferior retinectomy, perfluorocarbon drain, and silicone oil tamponade.
Postoperative positioning is crucial to ensure a successful retinal detachment repair; however, postoperative positioning may not be possible for older adults because of concomitant musculoskeletal disorders. The increased use of silicone oil in older patients in our series reflects both the greater complexity of the RRDs and the potential difficulties with postoperative positioning.
We also found that, although a greater number of elderly patients with an RRD underwent PPV alone, those who received SB plus PPV had a better single-surgery success rate (91% for SB plus PPV vs 74% for PPV alone, P = .03). Because most elderly patients have had cataract surgery, surgeons often prefer to tackle pseudophakic RRDs with PPV alone to prevent myopic shift and other potential SB-related issues. Although most patients have a favorable outcome with PPV alone, the addition of an encircling band may be beneficial in some patients.
Intraoperatively, the surgeon should manipulate the extraocular muscles carefully, as the oculocardiac reflex can result in arrythmias that can be particularly dangerous in geriatric patients with preexisting cardiac comorbidities.8 Additionally, because elderly patients are more likely to experience osteoarthritis and neuralgia, surgeons should avoid a prolonged surgery whenever possible.
WORSE OUTCOMES
Due to the increased complexity of both RRD presentation and surgical repair, the final outcomes of elderly patients with RRD are often worse than they would be in younger patients. In our cohort, we found that mean VA improved from 20/500 preoperatively to 20/125 postoperatively in the older patients, compared with 20/200 preoperatively to 20/40 postoperatively in the younger patients (P < .001). Single-surgery anatomic success rate was 78% in the older patients compared with 84% in younger patients (P = .03).
A previous study following patients over age 85 showed similar results.9 Nearly half of patients in that cohort who underwent PPV had a recurrent retinal detachment after repair (46%, n = 10/22), although the mean VA improved from 1.962 logMAR (20/1832) preoperatively to 1.232 logMAR (20/341) after a mean follow-up of 7.25 months.9
WRAP-UP
Although RRDs in the elderly have worse prognoses, there is still an improvement of quality of life that must not be discounted.10 Retinal detachment surgery remains effective in improving visual function in patients over age 80, but outcomes may not be as favorable as they are in younger patients. Preexisting comorbidities, delayed presentation, difficulties with postoperative positioning, and many other factors likely contribute to worse outcomes for RRD repair in the elderly. Thus, thoughtful and individualized approaches to the care of elderly patients with RRDs are recommended, especially considering that these clinical scenarios are becoming more common as our global population ages.
1. Ortmann JM, Velkoff VA. An aging nation: The older population in the United States. US Census Bureau. May 2014. Accessed June 30, 2021. www.census.gov/library/publications/2014/demo/p25-1140.html
2. Mitry D, Charteris DG, Fleck BW, Campbell H, Singh J. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. Br J Ophthalmol. 2010;94(6):678-684.
3. Patel SN, Starr MR, Obeid A, et al. Characteristics and surgical outcomes of rhegmatogenous retinal detachment in older adults: A multicenter comparative cohort study. Retina. 2021;41(5):947-956.
4. Klaver CC, Wolfs RC, Vingerling JR, Hofman A, de Jong PT. Age-specific prevalence and causes of blindness and visual impairment in an older population: the Rotterdam Study. Arch Ophthalmol. 1998;116(5):653-658.
5. Tielsch JM, Javitt JC, Coleman A, Katz J, Sommer A. The prevalence of blindness and visual impairment among nursing home residents in Baltimore. N Engl J Med. 1995;332(18):1205-1209.
6. Raczyńska D, Glasner L, Serkies-Minuth E, Wujtewicz MA, Mitrosz K. Eye surgery in the elderly. Clin Interv Aging. 2016;11:407-414.
7. Chow WB, Rosenthal RA, Merkow RP, et al. Optimal preoperative assessment of the geriatric surgical patient: a best practices guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. J Am Coll Surg. 2012;215(4):453-466.
8. Dallinger S, Findl O, Strenn K, Eichler HG, Wolzt M, Schmetterer L. Age dependence of choroidal blood flow. J Am Geriatr Soc. 1998;46(4):484-487.
9. Anteby R, Barzelay A, Barak A. Vitrectomy in patients 85 years of age and older: surgical outcomes and visual prognosis. Clin Interv Aging. 2018;13:243-249.
10. Ma Y, Ying X, Zou H, et al. Rhegmatogenous retinal detachment surgery in elderly people over 70 years old: visual acuity, quality of life, and cost-utility values. PLoS One. 2014;9(10):e110256.


-1_1638377570.jpg?auto=compress,format&w=70)



_1784132761.jpg?auto=compress,format&w=75)











