

AT A GLANCE
- There is no universally accepted approach to managing patients with optic pit maculopathy (OPM).
- The most common approach to OPM is vitrectomy, and advances in surgical techniques have made this approach safer and more effective.
- Regardless of technique, complete fluid resolution often takes more than a year, and patients must be educated on the expected postoperative course.
Optic disc pit (ODP) is a rare congenital disorder characterized by an excavation of the optic nerve head. These excavations typically appear at the temporal or inferotemporal segment of the optic disc, although central and nasal excavations have also been reported.1 ODP occurs in approximately one in 10,000 individuals with no racial or sex predilection. While most patients with ODP are asymptomatic, some can develop optic pit maculopathy (OPM), which is characterized by the presence of subretinal and intraretinal fluid extending from the pit into the macula. This can lead to progressive visual deterioration and usually presents in patients in their 30s and 40s.2,3
The exact pathogenesis of OPM remains unclear with significant debate on the origin of the subretinal and intraretinal fluid.4,5 Most believe that the source of the fluid is related to either the vitreous or the cerebrospinal fluid (CSF). For those who believe the fluid originates from the vitreous, it is postulated that vitreous traction on the macula allows fluid to enter the subretinal space through the optic pit more readily.6 Others argue that the fluid originates from the CSF through the subarachnoid space. Modern OCT imaging may suggest a connection between the subarachnoid space and ODP.7 This theory is further supported by a case report of silicone oil migration from the vitreous cavity into the intracranial space.8
MANAGEMENT OPTIONS
There is no universally accepted approach to managing patients with OPM. Early literature recommended conservative management, as spontaneous resolution of the fluid has been reported after a posterior vitreous detachment (PVD) develops.5,9 However, most patients will have chronic persistence of fluid with a risk for progressive central vision loss. Thus, retina specialists must be prepared to choose between several treatment approaches for OPM.
Laser photocoagulation to the temporal edge of the optic nerve is one of the earliest interventions reported—the theory being that a chorioretinal adhesion in the peripapillary region would prevent fluid from entering the subretinal space through the optic pit.10,11 This approach was limited by inconsistent results with low rates of complete fluid resolution. In addition, there is a risk for enlarging the blind spot by damaging the papillomacular bundle.10 The use of light laser burns can limit the damage to the nerve fiber layer.
Intravitreal gas injection is another minimally invasive approach that has been previously described. Injecting gas into the vitreous may be beneficial by inducing a PVD, alleviating vitreomacular traction, and even sealing the pit itself. Akiyama et al demonstrated a success rate of approximately 50%, but multiple injections were often necessary.12 Intravitreal gas injection can be combined with laser photocoagulation to potentially improve fluid resolution; using this technique, Lei et al had a 75% complete resolution rate of subretinal and intraretinal fluid, although some patients required repeat treatments.13
Theodossiadis et al described a macular buckling technique in which a scleral sponge is fixed externally in the area of the macula to reduce the anterior-posterior tractional forces. This technique showed a high rate of anatomical and functional success on long-term follow-up.14 However, the procedure is technically difficult with a steep learning curve and has not gained widespread use.
The most common approach to OPM is vitrectomy. Advances in surgical techniques—with the continued improvement of small-gauge, sutureless vitrectomy instrumentation—have made this approach safer and more effective. Because vitreous traction on the optic pit likely contributes to OPM, induction of a complete PVD during vitrectomy can be extremely beneficial.1,3,4 Staining of the hyaloid with triamcinolone can help to ensure complete hyaloid elevation during surgery (Figure 1). Vitrectomy also provides the opportunity to include other treatment modalities, such as endolaser, internal limiting membrane (ILM) peeling, and gas tamponade, to name a few.1,3,4 Some surgeons believe that laser photocoagulation to the edge of the temporal aspect of the optic pit can be more effective following vitrectomy.15 Others feel the laser is not necessary and remain concerned about possible complications.16 When performing endolaser at the time of the vitrectomy, surgeons can apply a lighter laser treatment in an attempt to reduce the risk of blind-spot enlargement (Figure 2).

Figure 1. To address vitreous traction on the optic pit, stain the hyaloid with triamcinolone to ensure complete hyaloid elevation during vitrectomy.
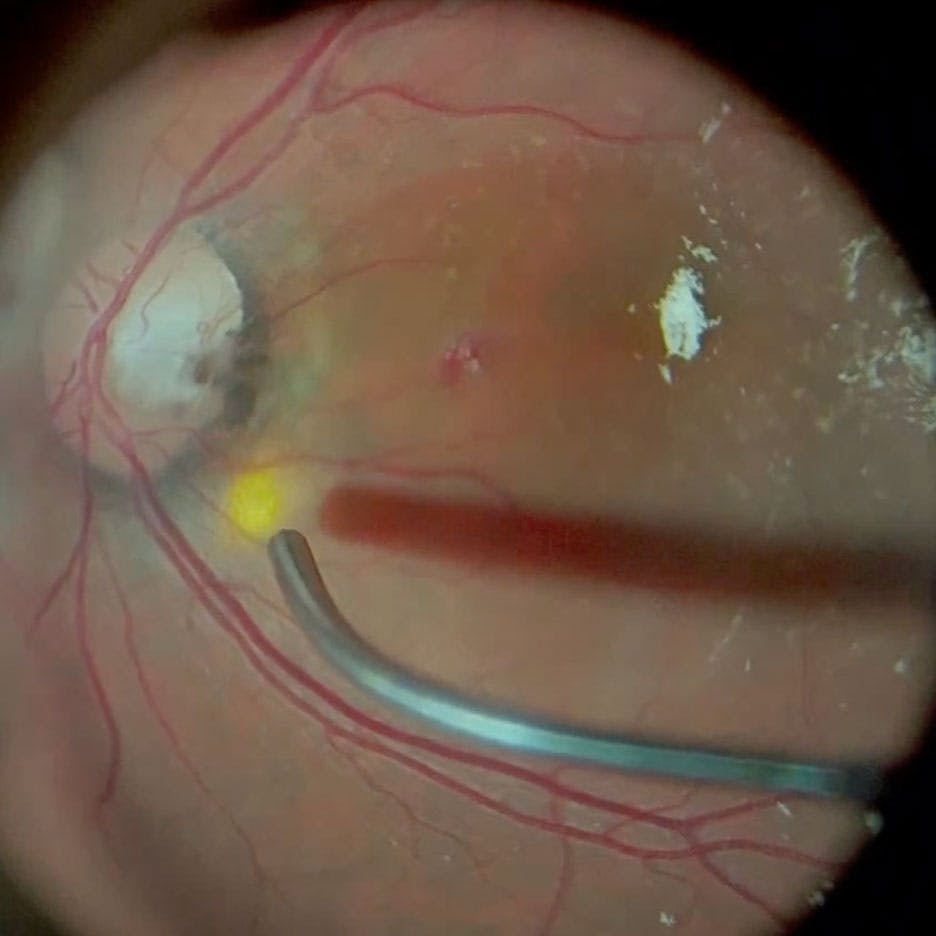
Figure 2. Surgeons can apply a single light-intensity row of laser at the temporal edge of the optic nerve to prevent fluid from entering the subretinal space.
Intraocular gas injection during vitrectomy may also enhance outcomes, as it can provide a longer-acting tamponade of the optic pit, facilitating resolution of the fluid. Adjuvant face-down positioning can further enhance the efficacy of the gas tamponade.
Some surgeons advocate for ILM peeling to further reduce tangential traction on the macula beyond hyaloid elevation alone.17 However, there is always a risk of causing a full-thickness macular hole with ILM peeling due to the thinned nature of the inner retinal layers.17,18 Several studies have shown successful management of OPM with vitrectomy without ILM peeling, and many surgeons choose to forego ILM peeling in these cases.15,19

A Case of Optic Pit Maculopathy
By Matthew A. Cunningham, MD, FASRS
Recently, numerous techniques have been described to cover or plug the pit at the time of surgery. Rather than a complete idiopathic macular pucker peel, some authors have advocated for creating an ILM flap that can be placed over or into the pit.20,21 Autologous scleral patch graft, amniotic membrane, autologous fibrin, and exogenous fibrin glue have all been described as ways to seal the optic pit.22-25 Although these modalities may result in faster resolution of the fluid, they do not necessarily provide better anatomical or visual outcomes. Each approach creates an added level of complexity or expense that must be compared with more traditional approaches.
SET EXPECTATIONS
When managing patients with OPM, patient education to set appropriate expectations is paramount. Regardless of surgical technique, we have found that complete fluid resolution often takes more than 12 months. The rate of visual improvement and the final visual outcome are also highly variable. Patients should be informed that multiple procedures may be necessary to achieve the best anatomical outcome.
Although ODP and OPM are rare conditions, retina specialists must be aware of the evolving management options. Many treatment approaches exist without any universally accepted standard. Understanding the potential benefits and limitations of each approach is necessary when deciding the optimal treatment for each patient.
1. Chatziralli I, Theodossiadis P, Theodossiadis GP. Optic disk pit maculopathy: current management strategies. Clin Ophthalmol. 2018;12:1417-1422.
2. Theodossiadis GP, Panopoulos M, Kollia AK, Georgopoulos G. Long-term study of patients with congenital pit of the optic nerve and persistent macular detachment. Acta Ophthalmol. 1992;70(4):495-505.
3. Georgalas I, Ladas I, Georgopoulos G, Petrou P. Optic disc pit: a review. Graefes Arch Clin Exp Ophthalmol. 2011;249:1113-1122.
4. Moisseiev E, Moisseiev J, Loewenstein A. Optic disc pit maculopathy: when and how to treat? A review of the pathogenesis and treatment options. Int J Retin Vitr. 2015;1:13.
5. Brown GC, Shields JA, Goldberg RE. Congenital pits of the optic nerve head. II. Clinical studies in humans. Ophthalmology. 1980;87(1):51-65.
6. Theodossiadis PG, Grigoropoulos VG, Emfietzoglou J, Theodossiadis GP. Vitreous findings in optic disc pit maculopathy based on optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2007;245(9):1311-1318.
7. Ohno-Matsui K, Hirakata A, Inoue M, Akiba M, Ishibashi T. Evaluation of congenital optic disc pits and optic disc colobomas by swept-source optical coherence tomography. Invest Ophthalmol Vis Sci. 2013;54(12):7769-7778.
8. Kuhn F, Kover F, Szabo I, Mester V. Intracranial migration of silicone oil from an eye with optic pit. Graefes Arch Clin Exp Ophthalmol. 2006;244(10):1360-1362.
9. Parikakis EA, Chatziralli IP, Peponis VG, Karagiannis D, Stratos A, Tsiotra VA, Mitropoulos PG. Spontaneous resolution of long-standing macular detachment due to optic disc pit with significant visual improvement. Case Rep Ophthalmol. 2014;5(1):104-110.
10. Theodossiadis G. Evolution of congenital pit of the optic disk with macular detachment in photocoagulated and nonphotocoagulated eyes. Am J Ophthalmol. 1977;84(5):620-631.
11. Taliantzis S, Perente A, Mitsi C, Panagiotopoulou, EK, Fotiadis I, Dardabounis D. Long-term follow-up of optic disc pit maculopathy treated with laser photocoagulation: a case report. Beyoglu Eye J. 2021;6(2):151-154.
12. Akiyama H, Shimoda Y, Fukuchi M, et al. Intravitreal gas injection without vitrectomy for macular detachment associated with an optic disk pit. Retina. 2014;34(2):222-227.
13. Lei L, Li T, Ding X, et al. Gas tamponade combined with laser photocoagulation therapy for congenital optic disc pit maculopathy. Eye (Lond). 2015;29:106-114.
14. Theodossiadis GP, Chatziralli IP, Theodossiadis PG. Macular buckling in optic disc pit maculopathy in association with the origin of macular elevation: 13-year mean postoperative results. Eur J Ophthalmol. 2015;25(3):241-248.
15. García-Arumí J, Guraya BC, Espax AB, Castillo VM, Ramsay LS, Motta RM. Optical coherence tomography in optic pit maculopathy managed with vitrectomy-laser-gas. Graefes Arch Clin Exp Ophthalmol. 2004;242:819-826.
16. Hirakata A, Okada AA, Hida T. Long-term results of vitrectomy without laser treatment for macular detachment associated with an optic disc pit. Ophthalmology. 2005;112:1430-1435.
17. Shukla D, Kalliath J, Tandon M, Vijayakumar B. Vitrectomy for optic disk pit with macular schisis and outer retinal dehiscence. Retina. 2012;32(7):1337-1342.
18. Rush RB, Simunovic MP, Aragon AV 2nd, Ysasaga JE. Postoperative macular hole formation after vitrectomy with internal limiting membrane peeling for the treatment of epiretinal membrane. Retina. 2014;34(5):890-896.
19. Avci R, Yilmaz S, Inan UU, et al. Long-term outcomes of pars plana vitrectomy without internal limiting membrane peeling for optic disc pit maculopathy. Eye (Lond). 2013;27(12):1359-1367.
20. Pastor-Idoate S, Gómez-Resa M, Karam S, et al. Efficacy of internal limiting membrane flap techniques with vitrectomy for macular detachment associated with an optic disc pit. Ophthalmologica. 2019;242(1):38-48.
21. Ravani R, Kumar A, Karthikeya R, Kumar P, Gupta Y, Mutha V, Singh S. Comparison of inverted ILM-stuffing technique and ILM peeling alone for optic disc pit-associated maculopathy: long-term results. Ophthalmic Surg Lasers Imaging Retina. 2018;49(12):e226-e232.
22. Khatri A, Shrestha SM, Prasai G, Pandit K, Bajgai P, Agrawal R, Gupta V. Minimally invasive procedure for optic disc pit maculopathy: vitrectomy with scleral plug and analysis on pattern of resolution. Scientific Rep. 2023;13(1):15724.
23. Rizzo S, Caporossi T, Pacini B, De Angelis L, De Vitto ML, Gainsanti F. Management of optic disk pit-associated macular detachment with human amniotic membrane patch. Retina. 2023;43(1):144-147.
24. Ozdek S, Ozdemir HB. A new technique with autologous fibrin for the treatment of persistent optic pit maculopathy. Retin Cases Brief Rep. 2017;11(1):75-78.
25. Soni A, Singh SR, Chhablani J. Fibrin glue for treatment of optic disc maculopathy. Saudi J Ophthalmol. 2021;34(3):227-229.


_1784132761.jpg?auto=compress,format&w=75)











