

AT A GLANCE
- Internal limiting membrane (ILM) flaps may be useful in cases of macular holes that are larger than 400 µm, chronic, present in high myopes, or that have failed traditional surgical techniques.
- Several common ILM flap techniques include inverted and temporal inverted flaps, retracting door and hinged flaps, cabbage leaf or star flaps, and free flaps.
- ILM flaps have become a valuable option for primary repair, with a higher reported closure rate of 93% compared with 74% for ILM peeling alone.
Macular hole (MH) surgery aims to release vitreoretinal tractional forces to close full-thickness defects of the foveal neurosensory retina. The conventional approach involves pars plana vitrectomy, lifting the hyaloid (if attached), internal limiting membrane (ILM) peeling, gas bubble placement, and postoperative head positioning.1 This well-established method is highly effective in patients with small- to medium- sized MHs (usually less than 400 µm), but cases of large, chronic, or refractory MHs remain a surgical challenge.2
ILM flaps may be useful in cases of more challenging holes, such as those that are larger than 400 µm, chronic holes, holes in high myopes, or MHs that have failed traditional surgical techniques. ILM flaps—which involve ILM peeling followed by placement of the residual ILM over the MH to promote closure3—are hypothesized to act as a scaffold for migration and proliferation of Müller cells, which secrete neurotrophic and growth factors that enhance the survival of retinal neurons.4 Since the first description of the inverted ILM flap in 2010,3 a variety of techniques have been developed and have shown favorable outcomes in MH closure and postoperative vision, making them a promising alternative for larger, chronic, and myopic MH. Here, we review several commonly used ILM flap techniques.
INVERTED AND TEMPORAL INVERTED ILM FLAPS
First introduced by Michalewska et al,3 the ILM flap is peeled in a circular fashion approximately 2 disc diameters around the MH but is left attached to the edges of the hole. After a segment of the peeled ILM is trimmed with vitreous cutters, the remaining central segment is gently massaged over the MH until the ILM is inverted to cover the hole.
The temporal inverted flap variation is created using the same method, but the ILM temporal to the fovea is peeled nasally so that the flap covers the hole during fluid-air exchange (Figure 1).5 This helps decrease the risk of dissociated optic nerve fiber layer.

Figure 1. The diagram depicts a temporal inverted ILM flap (A), while the surgical view (B) shows the stained ILM folded nasally (arrows) to cover the MH (asterisk). Surgical image courtesy of Avni P. Finn, MD, MBA.
RETRACTING DOOR AND HINGED FLAPS
The inverted ILM flap technique can be challenging in highly myopic eyes or those with posterior staphyloma because the flap is difficult to manipulate. Fluid-air exchange and fluid currents during surgery can also risk loss or displacement of the flap. The ILM retracting door technique was introduced as a technically easier procedure and allows for the confirmation of ILM placement over the MH.6
First, a Finesse Flex loop (Alcon) is used to create a large flap of ILM starting nasal to the MH. After the nasal edge is created, ILM forceps are used to peel the flap temporally over the fovea and temporal macula. The flap is then left attached temporally and draped back over the area of the hole. Thus, the previously taut ILM relaxes and retracts as it is draped back over the retina, allowing the nasal portion to cover the MH (Figure 2). Variations of the retracting door technique allow for hinging on various sides of the MH. For example, the ILM can be peeled to create a superior hinge to then drape back over the hole (Figure 3).
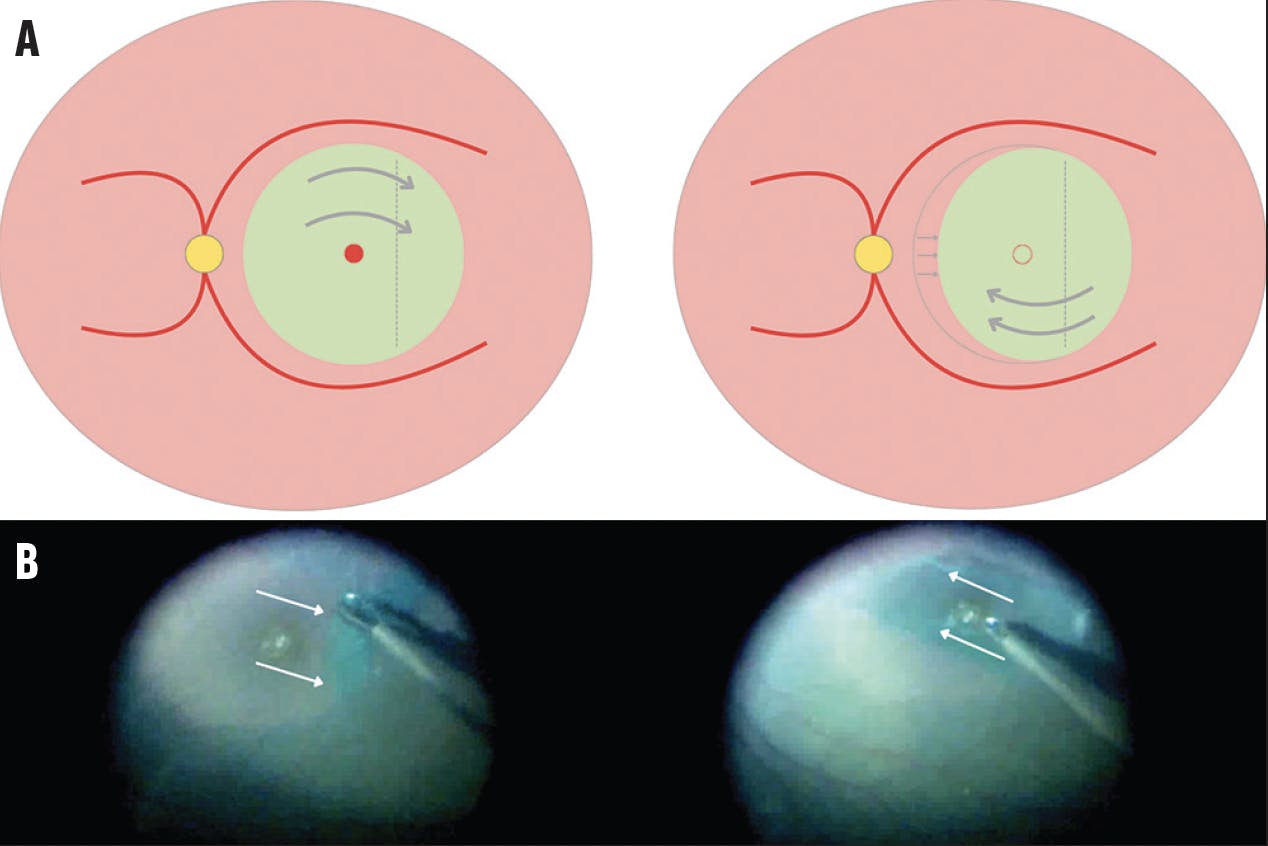
Figure 2. The diagram shows a retracting door flap, hinged temporally, which is peeled and placed back down to retract over the hole (A). The surgical view demonstrates peeling of the ILM temporally (arrows) followed by replacement over the hole (B). Surgical image courtesy of Avni P. Finn, MD, MBA.

Figure 3. The diagram shows a superiorly hinged retracting door flap (A). The surgical view demonstrates an ILM peel in the superior direction with a hinged fold (B, arrow). Surgical image courtesy of Prethy Rao, MD.
CABBAGE LEAF OR STAR FLAP
Instead of a circular ILM peel, the ILM can be peeled in separate areas to create three separate flaps with bases attached at the edge of the MH, creating a star-like shape.7 The flaps are trimmed and inverted over the macular hole, one on top of the other similar to the layers of a cabbage (Figure 4). This technique allows the flaps to stay over the hole and prevent displacement during fluid-air exchange.

Figure 4. The diagram of a cabbage leaf/star flap shows that the peeling is initiated in multiple directions, followed by placement of each arm of the flap over the hole (A). The surgical view shows the ILM peel directions (B, arrows) followed by the star configuration prior to placing the flaps over the MH (C, arrows). Surgical image courtesy of Avni P. Finn, MD, MBA.
FREE FLAP
When a hinged flap is not possible due to a prior ILM peel, a free flap may be a useful option. In this technique, a small piece of the ILM is peeled to create a free flap with a diameter similar to the MH and then placed inside the hole (Figure 5).8 Given the ILM’s affinity for the retina, surgeons should drag the flap across the retinal surface with a loop to the hole. A low molecular weight viscoelastic placed over the flap can stabilize it and avoid losing it in the eye. During fluid-air exchange, surgeons should dry slowly and keep the extrusion needle away from the macula. Challenges with the free flap include proper placement and frequent displacement during surgery or even postoperatively, although this may be ameliorated with perfluorocarbon liquids, viscoelastic plugs, or autologous serum as tissue adhesives.

Figure 5. These surgical views show the harvesting of an ILM segment away from the hole (A, arrow), visualization of the flap while held (B, circle), and placement of the flap over the MH (C). Surgical image courtesy of Avni P. Finn, MD, MBA.
BOOST YOUR CLOSURE RATES
Although ILM flaps are often reserved for large, myopic, or refractory full-thickness MHs that have failed ILM peeling, a recent review found that they are a valuable option for primary repair, with a higher reported closure rate of approximately 93% compared with 74% for ILM peeling alone as well as better postoperative visual acuity at 3 to 6 months.4 The researchers found that the odds of closure are particularly high for holes greater than 500 µm, although the benefit likely applies over a broad range of MH sizes. The same review also showed no significant differences between ILM flap techniques, suggesting general use of a flap in these cases is the key to maximizing the chances of a good outcome.4
No ILM peel is the same, and it is critical to adapt the flap to the circumstances of each individual case. Ensuring a thorough vitrectomy and posterior vitreous detachment is essential for a successful surgery, as is the use of dyes to help visualize the ILM. A familiarity with these techniques allows surgeons the necessary flexibility in their flap approaches to maximize anatomic and functional outcomes for each patient.
1. Rizzo S, Tartaro R, Barca F, Caporossi T, Bacherini D, Giansanti F. Internal limiting membrane peeling versus inverted flap technique for treatment of full-thickness macular holes: a comparative study in a large series of patients. Retina. 2018;38(1):S73-S78.
2. Frisina R, Gius I, Tozzi L, Midena E. Refractory full thickness macular hole: current surgical management. Eye. 2022;36(7):1344-1354.
3. Michalewska Z, Michalewski J, Adelman RA, Nawrocki J. Inverted internal limiting membrane flap technique for large macular holes. Ophthalmology. 2010;117(10):2018-2025.
4. Tzoumas N, McNally TW, Teh BL, et al. Internal limiting membrane flaps in macular hole surgery [published online ahead of print February 7, 2025]. Ophthalmol Retina.
5. Michalewska Z, Michalewski J, Dulczewska-Cichecka K, Adelman RA, Nawrocki J. Temporal inverted internal limiting membrane flap technique versus classic inverted internal limiting membrane flap technique: a comparative study. Retina. 2015;35(9):1844-1850.
6. Finn AP, Mahmoud TH. Internal limiting membrane retracting door for myopic macular holes. Retina. 2019;39(1):S92-S94.
7. Aurora A, Seth A, Sanduja N. Cabbage leaf inverted flap ILM peeling for macular hole: a novel technique. Ophthalmic Surg Lasers Imaging Retina. 2017;48(10):830-832.
8. Morizane Y, Shiraga F, Kimura S, et al. Autologous transplantation of the internal limiting membrane for refractory macular holes. Am J Ophthalmol. 2014;157(4):861-869.e1.




_1784132761.jpg?auto=compress,format&w=75)











