
AT A GLANCE
- When managing a patient with a dislocated IOL, it is advantageous to employ a technique that is applicable to a broad range of IOLs used by cataract surgeons.
- Almost all IOL styles can be repositioned with classic scleral fixation, with a few customized modifications.
- To modify the scleral suture technique for IOLs with silicone plate haptics, the Envista MX60 (Bausch + Lomb), or Raynor style IOLs, surgeons can use a handshake maneuver.
When vitreoretinal surgeons encounter a dislocated IOL, they have three management options: observe, exchange, or reposition.1,2 Observation is a viable option when the symptoms are minimal or if the fellow eye serves the patient’s needs. Many exchange techniques exist, with a general trend toward using posterior chamber techniques rather than exchanging for an anterior chamber IOL. Although many would consider scleral suturing, surgeons are also using newer approaches, such as using polytetrafluoroethylene (Gore-Tex, W.L. Gore) sutures to insert an Akreos IOL (Bausch + Lomb) or sutureless techniques involving externalizing a PMMA haptic (ie, the Yamane technique).3-5
Exchange techniques involve more surgical maneuvers, likely contributing to the risk of corneal decompensation. Perhaps more importantly, they involve an open repair, which may be more difficult in the setting of other ocular conditions. When the patient has a history of a corneal transplant or glaucoma surgery, an open repair presents additional risks and difficulties.
CHOOSING THE RIGHT TECHNIQUE
Thus, many retina surgeons may prefer IOL repositioning whenever possible. When there is sufficient residual anterior capsule, it is relatively easy to reposition the IOL into the sulcus, although that can introduce its own set of complications. When the dislocated IOL involves an endocapsular dislocation, the zonules and peripheral capsule are often too compromised to permit sutureless sulcus fixation.
When presented with a dislocated IOL, retina surgeons could benefit from having one technique that is applicable to a broad range of IOL styles. Focusing on one or two specific techniques enables the surgeon to hone the surgical steps and become more effective and efficient in the OR.
For me, that technique is scleral sutured IOLs, which has been reported and widely used for decades.1,2 Briefly, the technique involves looping the haptic with a 9-0 polypropylene suture (introduced with a 27-gauge needle 3 mm posterior to the limbus) through scleral flaps (usually placed at the 2 and 8 clock hour positions), tying externally while pinning the haptic internally, and later passing the polypropylene suture needle through the base of the flap to fixate the IOL (on both sides). This approach is well suited for three-piece IOLs (PMMA or acrylic optics) and even older one-piece PMMA IOLs (eg, CZ70BD [Alcon] style IOLs).
Here, I discuss minor modifications to the classic scleral suturing technique that allow its applicability to a much broader array of IOL types.
ONE TECHNIQUE, MANY LENSES
The Crystalens IOL (Bausch + Lomb) can be scleral sutured using the standard technique but requires a wider polypropylene suture loop to lasso the T-shaped haptic (Figure 1).6 A key element of the standard technique is to use intraocular forceps to grasp the optic and guide it through the loop. For the Crystalens, surgeons must first use the forceps to create more slack in the intraocular polypropylene loop-to-haptic complex. However, the Crystalens haptic complex is fragile and requires a gentler looping maneuver.

Figure 1. A rescued Crystalens IOL can be scleral sutured using the standard technique with a slightly wider polypropylene suture loop to lasso the broader haptic. Note that the lens haptics are fragile and require gentle handling. IOL image courtesy of Bausch + Lomb; suture added by author.
The standard scleral suture technique is easily adapted to one-piece acrylic IOLs such as the AcrySof SA60AT (Alcon) and other similar styles (Figure 2), despite their design for bag fixation (ie, shorter lateral dimension and non-independent haptic extensibility compared with three-piece IOLs with PMMA haptics).7 When adapting this technique to one-piece IOLs, avoid over tightening the initial knot that affixes the polypropylene to the haptic because it is easy for the suture to cut through the haptic (ie, cheesewire). An important modification is to internalize the haptic suture knot to suspend the IOL, as the lens dimensions are too small to pin the haptic to the eye wall without creating tilt. In addition, if the IOL is pulled too hard when pulling the IOL toward the opposite side, the suture can cut through the haptic. Other IOL designs use the same concept of some lens suspension.

Figure 2. The AcrySof SA60AT, although designed for bag fixation, can be scleral fixated; surgeons should allow the haptic suture knot to be internalized to suspend the IOL. IOL image courtesy of Alcon; suture added by author.
An important feature of any IOL that allows permanent fixation is for the haptic to be either long enough or have a reverse taper with the haptic being broader at the tip than at its apex. The Tecnis Symfony IOL (Johnson & Johnson) does not have this taper, so the modification for scleral suture fixation requires securing the polypropylene suture to the haptic proximal to the optic, taking advantage of the notch at the optic-haptic junction (Figure 3).8 While this requires the polypropylene suture be more internal, the distal haptics still function as spacers to avoid IOL twisting.
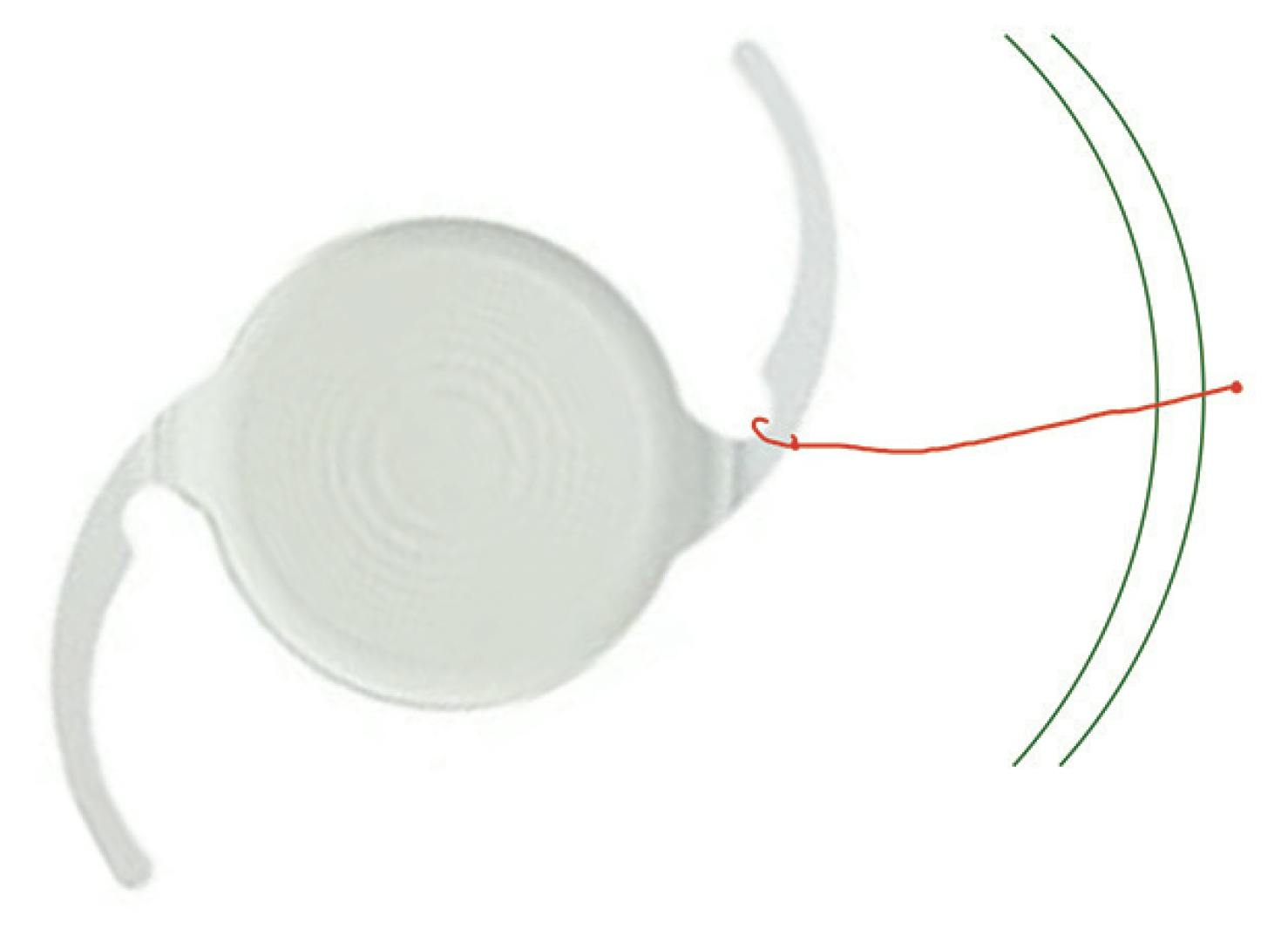
Figure 3. Because the Tecnis Symfony IOL does not have a reverse taper (ie, the haptic is broader at the tip than at the apex), surgeons must use the notch at the optic-haptic junction to secure the suture to the haptic proximal to the optic. IOL image courtesy of Johnson & Johnson; suture added by author.
Several other IOL designs can be scleral sutured with the right modifications. For IOLs with silicone plate haptics, the Envista MX60 (Bausch + Lomb), or Raynor style IOLs, surgeons can use a handshake maneuver in which the polypropylene suture-containing 27-gauge needle is directed through a hole in the haptic and the forceps holding the optic is released and used to grasp the suture (Figure 4).9 A separate, 25-gauge (or smaller) forceps is introduced anterior to the initial 27-gauge needle stab site to grab the suture from the first forceps (the handshake) and pulled externally. Then, the suture is temporarily tied until the other side is secured to allow the flexibility to center the optic. Although a similar technique can be used if there is a capsular tension ring, often it is better to remove the capsular tension ring and denude the haptics for repositioning.
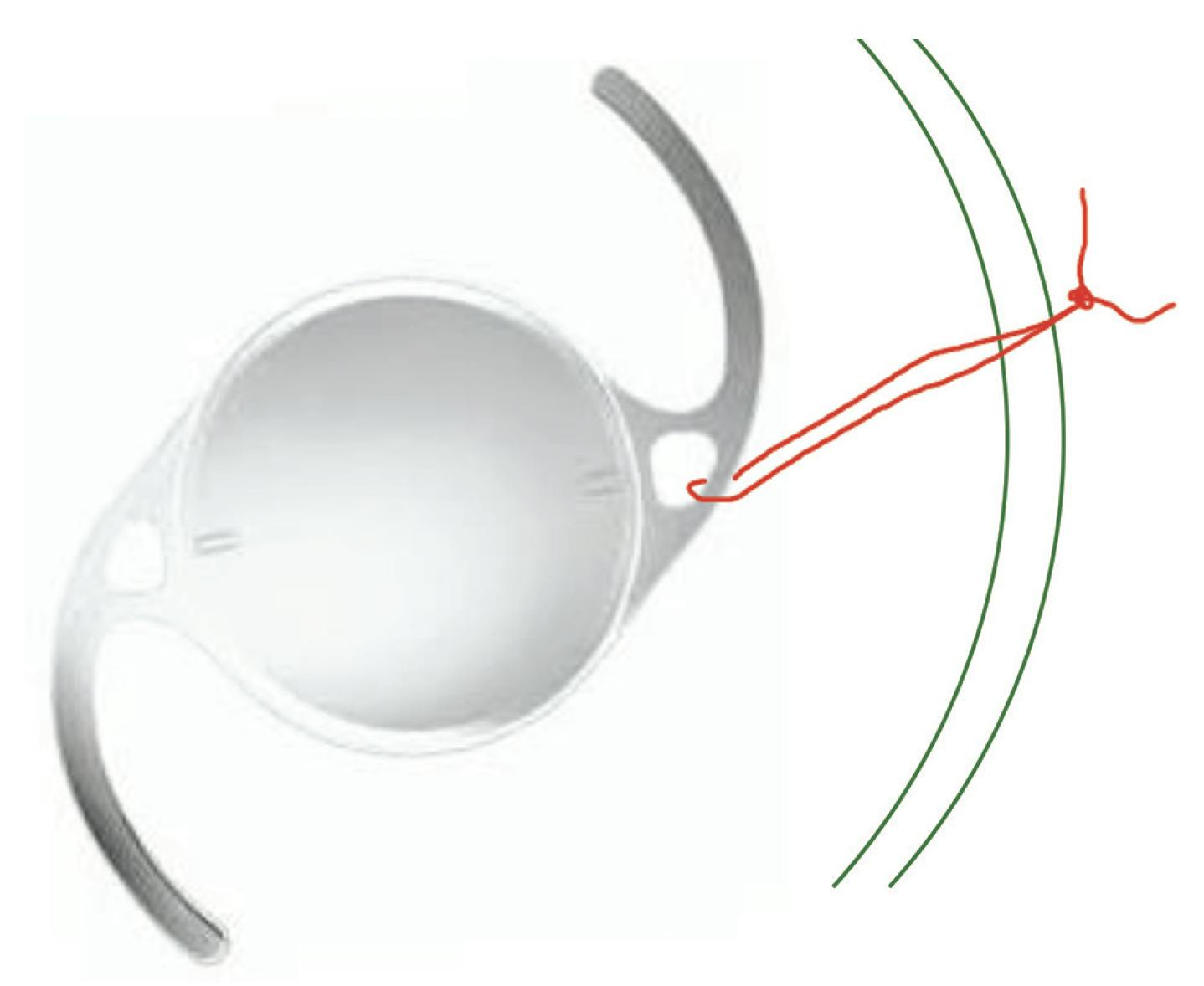
Figure 4. To scleral fixate the Envista MX60, surgeons can use a handshake maneuver to suture through a hole in the haptic. IOL image courtesy of Bausch + Lomb; suture added by author.
For IOL designs without holes, the initial polypropylene-containing 27-gauge needle can be used to pierce the IOL at the broader zone at the optic-haptic junction and a similar handshake maneuver pursued (Figure 5).

Figure 5. To reposition the Aspira IOL (HumanOptics)—which has no holes and has a tapered haptic—surgeons can use the piercing or impaling modification. IOL image courtesy of HumanOptics; suture added by author.
The Akreos IOL can be scleral fixated with a similar handshake maneuver but requires another modification to use the holes in all four haptics (Figure 6).10 The polypropylene-containing 27-gauge needle is introduced through a partial-thickness radial scleral incision about 2 clock hours from the scleral flap, directed through one haptic hole, and grasped by the first intraocular forceps. The second forceps is introduced through the base of the usual scleral flap through the hole in the second haptic on that side, the handshake maneuver is used to take the suture from the first forceps, and the non-needled end is withdrawn from the eye. Then, the needled end of the suture is at the stab incision through the radial scleral incision; it is grasped with a needle driver and passed intrasclerally to the partial-thickness scleral flap, where the ends are then tied (temporarily until the other side is tied to center the optic).

Figure 6. When rescuing an Akreos lens with scleral fixation, surgeons can use a modified handshake technique to use the holes in each of the four haptics. IOL image courtesy of Bausch + Lomb; suture added by author.
REPLACE OR RESCUE
IOL rescue is not ideal when there is a damaged or broken haptic or if the patient is on tamsulosine (Flomax, Sanofi), which carries a risk of subsequent uveitis-glaucoma-hyphema syndrome and could ultimately require IOL exchange.11,12
If you are rescuing a lens, almost all styles of dislocated IOLs can be repositioned with the same base scleral fixation technique, but with a few customized modifications. Master the classic approach and just a few tricks in the OR, and you can ensure a smooth IOL rescue, no matter the lens.
Author disclaimer: These techniques are considered off-label for these lenses.
1. Smiddy WE, Ibanez GV, Alfonso E, Flynn HW Jr. Surgical management of dislocated intraocular lenses. J Cat Ref Surg. 1995; 21(1):64-69.
2. Kim SS, Smiddy WE, Feuer W, Shi W. Management of dislocated intraocular lenses. Ophthalmology. 2008; 115(10):1699-1704.
3. Khan MA, Gerstenblith AT, Dollin ML, Gupta OP, Spirn MJ. Scleral fixation of posterior chamber intraocular lenses using gore-tex suture with concurrent 23-gauge pars plana vitrectomy. Retina. 2014;34(7):1477-1480.
4. Prenner JL, Feiner L, Wheatley HM, Connors D. A novel approach for posterior chamber intraocular lens placement or rescue via a sutureless scleral fixation technique. Retina. 2012;32(4):853-855.
5. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-1142.
6. Smiddy WE. Crystalens repositioning with scleral suture technique. Retinal Case Brief Rep. 2021;17(3):231-232.
7. Leung EH, Mohsenin A, Smiddy WE. Scleral suture fixation technique for one-piece acrylic intraocular lens. Retina Case Brief Rep. 2016;12(3):251-253.
8. Echegaray JJ, Smiddy WE. Scleral suture fixation of dislocated posterior chamber intraocular lens: modification for tapered haptics. Retina. 2023;43(6):1039-1040.
9. Smiddy WE. Scleral suture fixation for dislocated silicone plate haptic intraocular lens. J Retina Vit Dis. Retina. 2023;43(12):2057-2058.
10. Fan KC, Smiddy WE., Rescuing an Akreos 4-Point Haptic Intraocular Lens: A novel surgical technique. Retina. 2021;43(9):1616-1619.
11. Patel NA, Gangasani N, Yannuzzi NA, Melo G, Flynn HW, Smiddy WE. Indications and outcomes for the removal of intraocular lens implants in a retinal surgery practice. Ophthalmic Surg Lasers Imaging Retina. 2019;50(8):504-508.
12. Elhusseiny AM, Lee RK, Smiddy WE. Surgical management of uveitis-glaucoma-hyphema syndrome. Int J Ophthalmol. 2020;13(6):935-940.




_1784132761.jpg?auto=compress,format&w=75)











