

Every Friday in the retina clinic is Friday the 13th, regardless of what the calendar says. A Friday last December was no exception, when a macula-on retinal detachment (RD) was added to the schedule. A 62-year-old woman presented with a complaint of seeing “a curtain” in her right eye vision for the past day. The kicker was that she also reported a severe allergy to all eye drops. Her allergy was more than itching and hives—she reported previous anaphylactic reactions to eye drops. A deeper dive into her medical history revealed that the preservative benzalkonium chloride was the likely culprit. Because Friday afternoon was already hectic, and we didn’t want to test our resuscitation skills, we deferred use of any eye drops, including for IOP testing.
This presentation, a classic RD, usually prompts a cascade of surgical decisions. Who is available to operate? Should we handle it over the weekend or can it wait until Monday? Instead, we faced a far bigger problem with this patient: How could we diagnose, much less repair, an RD without dilating the patient?
In this article, we walk you through the myriad dilemmas and decision points we faced, hoping to provide a roadmap to help you successfully navigate similar cases you may encounter in the future.
DIAGNOSTIC CHALLENGE
Ultra-widefield fundus imaging (Optos), a controversial purchase within our practice due to cost, was a lifesaver, as it captured a superonasal RD through an undilated pupil (Figure 1). The detachment repair could wait up to 3 days (until the following Monday), but first we needed to decide where to perform the surgery.

TIMING ISSUES
We typically operate at one of several outpatient ambulatory surgery centers (ASCs). For this patient, however, we felt that a hospital setting, with the ICU down the hall, would be better in case she had a severe anaphylactic reaction requiring respiratory support.
The patient was pseudophakic, and we knew she had been dilated 5 and 6 months prior for cataract surgery, with preservative-free drops ordered by her surgeon a few weeks before the elective surgery. This was not possible to achieve over the weekend for our urgent RD surgery. None of our local compounding pharmacies stocked preservative-free dilating drops, and we were referred to several out-of-state pharmacies that could provide the drops in 1 or 2 weeks, which was too long a delay for a macula-on RD.
Our first thought was to refer the patient to the local university eye department and let them sort it out. Their pharmacy might have preservative-free eye drops readily available, and they had the hospital backing them up for any allergy issues. However, we knew they would face the same issues we faced, possibly with no better solutions.
We decided to schedule the patient at the hospital for early Sunday morning, when it was usually calm and the critical care team would be best equipped to handle any complications before, during, or after surgery. We spent our Saturday discussing the case with the nursing supervisor, pharmacist, hospitalist, and anesthesiologist.
One proposal was to admit the patient the day before to receive intravenous steroids, but she declined this due to a previous reaction to systemic steroids. The patient was insistent on outpatient surgery with no hospital admission.
SURGICAL STEPS
Pretreatment with diphenhydramine (Benadryl, Johnson & Johnson) was the next best option. We had no choice but to dilate her, for which we used two sets each of topical cyclopentolate 0.5% and phenylephrine 2.5%, with digital punctal occlusion and closed eyelids to minimize systemic absorption. Her eye dilated beautifully with no reaction.
Other options we considered using if the patient could not be dilated included iris hooks (the hospital never heard of and didn’t stock), a Malyugin ring (Labtician Ophthalmics; we had no experience with), or intracameral preservative-free epinephrine in hope that this would dilate the pupil adequately. With modern wide-angle viewing systems, a large pupil, although nice, isn’t essential for retina surgery.
The surgery was performed under local anesthesia with sedation. For the block, we used preservative-free bupivacaine 0.75%. The 25-gauge vitrectomy with endolaser and SF6 gas injection was uneventful. The patient was able to receive the standard subconjunctival cefazolin and dexamethasone, both also preservative-free.
POSTOPERATIVE PICTURE
In the recovery room, the patient had no significant allergic reaction other than mild redness and itching. She was discharged to home with diphenhydramine for prophylaxis against any delayed reaction.
The next day in the office, we deferred an IOP check. Fortunately, she was still dilated from surgery. She had drops left over from her cataract surgery—preservative-free difluprednate and fortified gentamicin—both of which would suffice, given the urgency of her case and our inability to order new drops on such short notice, and we instructed her to used them four times a day for 2 weeks.
For subsequent postoperative dilation and IOP checks, we used a compounded preservative-free combination of cyclopentolate, ketorolac, phenylephrine, and tropicamide. This was likely excessive, but it was available from an out-of-state compounding pharmacy and was effective. We ordered the unit dose vials delivered to the patient for future visits with us or any other eye care provider.
Four months after surgery, the patient’s VA was 20/20 OD, and subsequent monitoring was performed with ultra-widefield imaging (Figure 2).
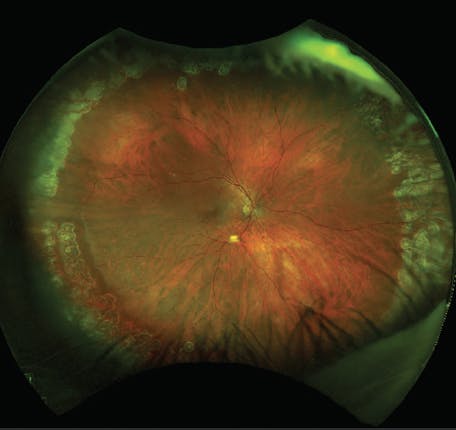
Figure 2. With careful planning, the patient had a successful outcome with no signs of allergic reaction to the medications used for her retinal detachment repair.
TAKE-HOME POINTS
The patient had a great result, and we were able to work around her severe eye drop allergy. If you encounter a similar case, keep the following pearls in mind.
- Preservative allergy is uncommon, but it can be severe.
- If surgery or other treatment is needed acutely, consider using commercially available preservative-free eye drops and medications. Compounding pharmacies may require 1 or 2 weeks of lead time, making them useful options for elective but not for urgent surgery.
- Although many retina specialists prefer the ASC setting for surgery, hospitals provide a valuable backup if medical conditions come into play that require a higher level of care. Make use of medical consultants who may also have suggestions or ideas.
- Nonmydriatic imaging, although not ideal, is a useful option when dilation isn’t possible, for whatever reason.
Even in the heat of the moment, a few minutes of calm thoughtfulness can help you see the right path forward to achieve a positive experience for you and the patient.






_1784132761.jpg?auto=compress,format&w=75)











