


There are significant anatomical differences between pediatric and adult eyes that have important implications for pediatric vitreoretinal surgery. For example, posterior segment volume is less than 50% at birth, and axial length is approximately 70% compared with an adult eye.1 Pars plana width is an important consideration to avoid injury to the lens or retina during trocar placement. The infant lens is thicker and more spherical, and the lens-to-globe ratio is greater in children.2 The hyaloid is very adherent to the retina in young children, and vitreous removal may be difficult.3 Here, we highlight a variety of surgical considerations in pediatric cases.
AT A GLANCE
- Obtaining informed consent from the child’s legal guardian is a fundamental part of preoperative care.
- Inducing a posterior vitreous detachment can be one of the most challenging steps during pediatric vitreoretinal surgery.
- In pediatric eyes, less is more, and aggressive surgical manipulation may not be necessary to achieve the planned surgical goals.
PREOPERATIVE CARE
Obtaining informed consent from the child's legal guardian is a fundamental part of preoperative care. Vitreoretinal surgeons should have a thorough discussion with the legal guardian and caretakers regarding important aspects of perioperative care. Parents should have realistic expectations about the visual prognosis of their child, and they should be educated on the difference between anatomical and functional success. Necessary postoperative care, including compliance with postoperative visits, eye drops, and pain management, should be emphasized.
In clinic, if imaging is not possible or provides inadequate anatomical information, examination under anesthesia (EUA) should be considered prior to any surgery. Surgeons should have a low threshold to perform EUA in the setting of pediatric vitreoretinal disorders. A thorough slit lamp and dilated fundus examination should be performed. OCT and widefield imaging can also be helpful in the preoperative evaluation of pediatric patients. Examination of the fellow eye is critical because bilateral surgery or prophylactic treatment of the other eye may be needed in select cases.
INTRAOPERATIVE CONSIDERATIONS
Scleral Buckles
These remain an essential therapeutic tool in children with retinal detachment (RD). Scleral buckles can be a primary procedure or in combination with vitrectomy, and most rhegmatogenous RDs in children should be approached initially with a scleral buckle (Figure 1), especially in eyes with a clear lens, anterior breaks, and absence of proliferative vitreoretinopathy (PVR).4 In recent years, scleral buckles have been used less frequently for tractional RDs, such as in the setting of retinopathy of prematurity, given the advances in vitrectomy machines.1
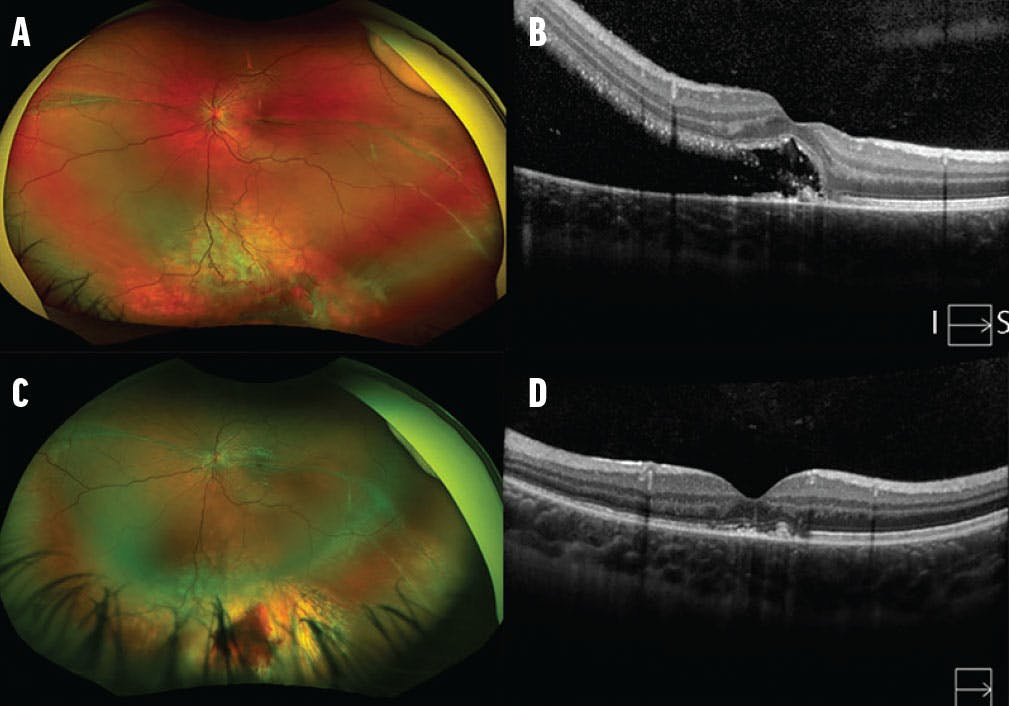
Figure 1. A 5-year-old girl was referred for evaluation of macular fold and noted to have a chronic inferior rhegmatogenous RD with an inferior break and demarcation line through the fovea (A). The patient underwent primary scleral buckle with silicone band and cryotherapy. Preoperative SD-OCT imaging with vertical cut (inferior to superior) demonstrated foveal splitting and a demarcation line (B). Four months after surgery, the peripheral break is surrounded by cryotherapy scars and the retina is attached (C, D).
After scleral buckling, postoperative considerations in children range from refractive and sensory amblyopia to strabismus and alterations in eye growth. Patients should be routinely followed during the postoperative period by their retina specialist and pediatric ophthalmologist. In younger pediatric patients, scleral buckle revisions are often required to compensate for a growing eye. It is preferable to divide rather than remove buckle elements because the encapsulated explant can provide continued support for the retina and vitreous base.5
Surgical Approach
In cases of advanced RD and/or vitreous opacities, lens-sparing vitrectomy may be necessary to release tractional components or clear vitreous opacity. In cases of lenticular opacities or anterior retinal drag, a translimbal approach with combined lensectomy and vitrectomy may be preferable.
Trocar Placement
There are several methods for placing trocars in pediatric eyes. One method adheres to a standard age-adjusted nomogram (Table).6 Because the pars plana is not fully developed until 8 or 9 months of age, the pars plicata approach with incisions within 0.5 mm to 1 mm posterior to the limbus is preferred in the infant eye.7 For eyes with unusual anatomy, such as microphthalmos, or eyes with severe anterior segment abnormalities, transscleral illumination is another useful method to determine the location of the pars plana for safe sclerotomy entry.

Trocars and instruments should be inserted perpendicular to the sclera and parallel to the visual axis. Given the increased elasticity and reduced rigidity, entering the pediatric eye is often challenging and may require twisting maneuvers with persistent pressure and counter traction with a second instrument.1
PVD Induction
In pediatric patients, there is firm adherence of the cortical vitreous to the retina. Therefore, inducing a posterior vitreous detachment (PVD) can be a challenging step during pediatric vitreoretinal surgery. Typically, PVD induction is indicated for young patients in cases involving traumatic macular hole repair, epiretinal membrane peeling, or RD repair or to address a vitreous opacity, such as vitreous hemorrhage. Failing to induce a PVD in these cases may lead to poor surgical outcomes.8
We recommend a stepwise approach by starting the PVD induction with chromovitrectomy with diluted triamcinolone acetonide (Figure 2, Video 1). For particularly adherent vitreous, we use a flexible loop (Alcon) or a bimanual technique using a lighted pick and the vitreous cutter. Once the flex loop touches the retina to engage the posterior hyaloid, the hyaloid is separated from the optic disc and peripapillary retina using gentle radial motions. We aspirate with the cutter over the area near the optic nerve and gently lift the induced edge with the lighted pick from the other end. Perfluorocarbon liquid is helpful for a partially induced PVD, particularly in the setting of macular RD. Perfluorocarbon liquid is gently infused through the opening created in the hyaloid and over the optic nerve to help lift the PVD.
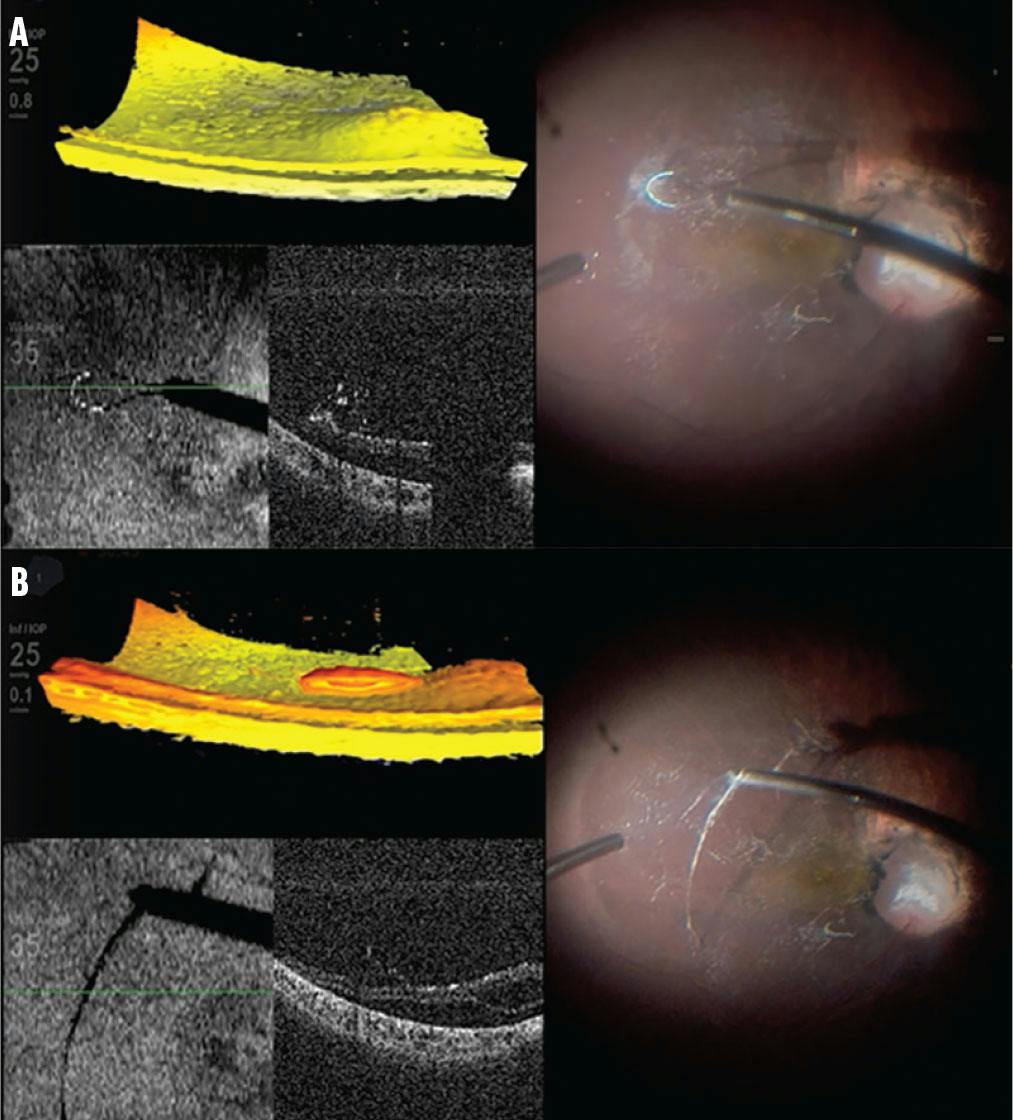
Figure 2. During PVD induction, after highlighting the posterior hyaloid with diluted triamcinolone acetonate, the flex loop is employed to engage and lift the posterior hyaloid with radial movements (A). The hyaloid is seperated from the peripapillary retina with vitreous cutter suction (B).

Video 1. Inducing a Posterior Vitreous Detachment in a Pediatric Patient.
Occasionally, a PVD can be propagated to the periphery, but it is important to avoid causing retinal breaks. A compromise is a judicious core vitrectomy that leaves a layer of cortical vitreous on the retina that is as thin as possible. If complete removal of the vitreous from the periphery is not feasible, a thorough shaving procedure becomes essential.5
Lens Management
Recent advances in pediatric vitreoretinal surgery techniques have improved the anatomic and visual outcomes for lens-sparing vitrectomy, and this is the preferred method in most pediatric cases. The main advantage is the preservation of the refractive state of a phakic eye to facilitate visual rehabilitation and development. Lensectomy is recommended for addressing most anterior retinal pathologies or in eyes at high risk for PVR, such as severe globe injury or uveitis.5 In cases of retinal pathology with advanced PVR, capsular remnants may serve as a scaffold for preretinal proliferation and circumferential vitreoretinal contraction or development of synechiae with distortion of the pupil. Therefore, complete removal of the capsular remnants should be attempted.9 If lensectomy is planned, some or all the trocars can be placed at the limbus to minimize trocar manipulation of the pars plana. The pediatric crystalline lens is generally soft enough to aspirate with a vitrector.
VITRECTOMY TIPS
In pediatric eyes, less is more (Figures 3 and 4, Video 2). Aggressive surgical manipulation may not be necessary to achieve the planned surgical goals. Iatrogenic breaks often result in severe PVR, causing a catastrophic outcome with inoperable RDs. In eyes with PVR, it is preferable to perform segmentation instead of delamination when removing preretinal membranes due to the firm vitreoretinal attachments in children.10

Figure 3. An 11-month-old girl with incontinentia pigmenti and previous history of retinal photocoagulation presented with a temporal ridge and superotemporal tent-like tractional RD in the left eye (A). During the vitrectomy, using the vitreous cutter, vertical scissors, and Maxgrip forceps (Alcon), the posterior hyaloid was carefully peeled and segmented bimanually to avoid the creation of retinal tears. Two months after surgery, the traction was relieved from the optic nerve, and the macula and the retina were relaxed and reattached (B).

Figure 4. During the lens-sparing pars plana vitrectomy for the patient in Figure 3, vertical scissors (A) and a vitreous cutter (B) were used to carefully segment and delaminate the posterior hyaloid membrane from the underlying detached macula. An additional trocar was inserted to facilitate bimanual dissection of tractional membranes (C).

Video 2. Vitrectomy in a Child with Incontinentia Pigmenti.
Posterior drainage retinotomies are best avoided, as extensive fibrous proliferation can occur postoperatively, leading to RD.
Choice of Tamponade
Intraocular gas can be challenging to use in children, given the difficulties with positioning and IOP monitoring.11,12 However, gas—especially longer-acting gases—may still be the best tamponade, with silicone oil (either 1,000 cs or 5,000 cs) reserved for patients who have inferior pathology or need a longer tamponade (Figure 5). Pediatric patients may maintain intraocular silicone oil for a prolonged time. The tamponade choice and its risks and benefits should be discussed thoroughly with the patient's caregiver.

Figure 5. A 12-year-old boy with Stickler syndrome presented with total rhegmatogenous RD of the right eye with two equatorial giant retinal tears (A). The patient underwent 25-gauge pars plana vitrectomy with endolaser and 1,000 cs silicone oil tamponade. Five years after surgery, the retina is attached (B) with excellent macular anatomic reattachment seen on SD-OCT (C).
Closure
Surgeons should suture the sclerotomies at the completion of the surgery to minimize the risk of hypotony, tamponade loss, and infection. Closure of the sclera and conjunctiva may be done with absorbable 8-0 or 9-0 vicryl or plain gut sutures.
POSTOPERATIVE CARE
It is essential to schedule regular postoperative examinations. The primary purpose of postoperative care is to support visual and anatomical rehabilitation and monitor for other conditions, such as cataract, glaucoma, recurrent RD, epiretinal membrane, inflammation, infection, amblyopia, strabismus, diplopia, and ptosis. Refractive issues may need to be addressed with glasses, contact lenses, or patching. Working closely with a pediatric ophthalmologist is crucial to provide comprehensive care. It is important to discuss postoperative positioning, eye drops, and pain management because compliance can be an issue in pediatric patients.
WORTH THE CHALLENGE
Pediatric vitreoretinal surgery can be challenging but extremely rewarding by potentially helping to restore vision and function in a child. Pediatric patients often cannot communicate their thoughts or feelings, and it becomes even more crucial to have a thorough discussion with the patient’s caretaker about what to expect during surgery and postoperative instructions.
1. Özdek Ş, Berrocal A, Spandau U. Pediatric Vitreoretinal Surgery. Springer International Publishing; 2023.
2. Augusteyn RC. On the growth and internal structure of the human lens. Exp Eye Res. 2010;90(6):643-654.
3. Sebag J. Age-related differences in the human vitreoretinal interface. Arch Ophthalmol. 1991;109(7):966-971.
4. Wenick AS, Baranano DE. Evaluation and management of pediatric rhegmatogenous retinal detachment. Saudi J Ophthalmol. 2012;26(3):255-263.
5. Sadda SVR, Schachat AP, Wilkinson CP, et al. Ryan’s Retina. Elsevier Health Sciences; 2022.
6. Wright LM, Harper CA 3rd, Chang EY. Management of infantile and childhood retinopathies: optimized pediatric pars plana vitrectomy sclerotomy nomogram. Ophthalmol Retina. 2018;2(12):1227-1234.
7. Hairston RJ, Maguire AM, Vitale S, Green WR. Morphometric analysis of pars plana development in humans. Retina. 1997;17(2):135-138.
8. Vajzovic L, Thomas A. Tips for inducing posterior vitreous detachment in young patients. Retinal Physician. March 2017. Accessed September 5, 2023. www.retinalphysician.com/newsletter/surgical-maneuvers/march-2017
9. Ranchod TM, Capone A Jr. Tips and tricks in pediatric vitreoretinal surgery. Int Ophthalmol Clin. 2011;51(1):173-183.
10. Gan NY, Lam WC. Special considerations for pediatric vitreoretinal surgery. Taiwan J Ophthalmol. 2018;8(4):237-242.
11. Berrocal A, Trese M. Pearls for pediatric retina surgery. Retina Today. 2023;10(3):34.
12. Fekrat S. The Duke Manual of Vitreoretinal Surgery. Wolters Kluwer; 2020.





_1784132761.jpg?auto=compress,format&w=75)











