

AT A GLANCE
- Data from the DISCOVER trial showed that using intraoperative OCT (iOCT) during posterior segment surgery added valuable information in roughly 60% of cases, regardless of surgeon experience.
- iOCT has been applied during epiretinal membrane peeling to visualize the membrane and minimize the use of adjuvant dye.
- iOCT can provide real-time feedback during vitreoretinal surgery, but more investigation is needed to determine its ability to affect outcomes.
OCT has had profound clinical implications since its invention in 1991.1 Now, with the advent of the microscope-integrated platform, we see an increased use of intraoperative OCT (iOCT).1,2 The PIONEER (531 eyes) and DISCOVER (837 eyes) studies provided surgeons with detailed information on the utility of iOCT in anterior and posterior segment surgeries.3,4 DISCOVER’s 3-year results showed that the use of iOCT during posterior segment surgery added valuable information in approximately 60% of cases and potentially altered surgical decision making in approximately 30% of cases, regardless of surgeon experience.3 Here, we present an overview of five vitreoretinal surgical scenarios where iOCT can be helpful.
SCENARIO NO. 1: VITREORETINAL INTERFACE DISORDERS
iOCT can help to modify surgical decision making because it can reveal either residual membranes or completion of the membrane peel—potentially avoiding incomplete treatment or unnecessary surgical maneuvers.5
Macular hole (MH) surgery performed with iOCT has been reported to yield a high single-surgery success rate. In a post-hoc analysis of the DISCOVER trial, single-surgery MH closure was achieved in 97.6% of cases, comparable to outcomes in eyes receiving pars plana vitrectomy and internal limiting membrane (ILM) peel without iOCT (87% to 97%).5-7
Analysis of the MH morphology after the iOCT-assisted ILM peel can reveal features capable of predicting better anatomic and functional outcomes.8,9 For example, in a retrospective case series of MH patients who were evaluated with iOCT at the end of the ILM peel, patients with a large MH (> 400 µm) and the presence of a “hole-door” (vertical pillars of tissue projecting into the vitreous cavity after ILM peeling) or “foveal flap” (preoperative foveal flap that adhered to the hole edge after ILM peeling) configuration had significantly better final visual acuity and restoration of the external limiting membrane.8
A post-hoc analysis of eyes from the PIONEER trial undergoing full-thickness MH repair demonstrated that intraoperative decrease in MH volume, intraoperative changes in minimal width, and pre-incision minimal width were the strongest predictors for early MH closure.9
iOCT has been applied during epiretinal membrane (ERM) peeling to visualize the membrane and minimize the use of adjuvant dyes such as ICG, which can potentially be associated with retinal toxicity.10-13 Other advantages of iOCT include being able to verify the absence of intraoperative full-thickness MHs or residual membrane in surgeries for ERM or vitreomacular traction, which might affect the tamponade choice (Figure 1).14,15 iOCT can reveal remnant posterior vitreous cortex that is strongly adherent to the retinal surface—particularly in highly myopic eyes with foveoschisis—and can reveal altered foveal architecture after the peel.16,17

Figure 1. The preoperative OCT image shows vitreomacular traction (A), and the iOCT confirmed a complete membrane peel without a residual full-thickness retinal defect (B).
Image courtesy of Aleksandra V. Rachitskaya, MD. FASRS
Despite these advantages, further investigation is needed to understand the utility of iOCT to improve anatomical and functional outcomes, single-surgery success rate, and intraoperative efficiency.
SCENARIO NO. 2: SUBMACULAR SURGERY
iOCT has been shown to be useful in subretinal bleb creation.18,19 This becomes even more paramount in inherited retinal diseases where a bleb is created in the macula (Figure 2). Many patients with inherited retinal diseases have atrophic retinas, which can make it difficult to induce a localized detachment with balanced salt solution (BSS) or gene therapy product. iOCT can help to confirm that the injection occurs in the subretinal space, as opposed to damaging the underlying retinal pigment epithelium (RPE) or injecting into the sub-RPE space. With a BSS pre-bleb, iOCT can help localize the bleb retinotomy site and allow for optimal positioning of the subretinal cannula with gene product into the subretinal space. Following the delivery of the viral vector, iOCT can help to verify that a full-thickness MH did not develop.18 In addition to visualizing the retinal architecture, novel research is measuring the volume of the bleb to determine the exact treatment delivered.20

Figure 2. When delivering subretinal gene product, iOCT is used to confirm foveal inversion with no MH formation.
Image courtesy of Aleksandra V. Rachitskaya, MD. FASRS
Other subretinal pathology can be accessed with the assistance of iOCT, including subretinal PFO. iOCT can aid in visualizing subretinal PFO, confirming complete PFO removal, and ensuring there is no residual MH formation or other retinal defect.21 In instances of submacular hemorrhage, iOCT can be useful in identifying optimal needle placement for the subretinal injection of tissue plasminogen activator, preventing intraretinal or sub-RPE injection.22
SCENARIO NO. 3: PROLIFERATIVE DIABETIC RETINOPATHY
When operating on patients with proliferative diabetic retinopathy (PDR), there is often severely altered tissue anatomy that requires delicate manipulation and clear delineation of surgical planes. Common sight-threatening complications of diabetes in patients with PDR include nonclearing vitreous hemorrhage, tractional retinal detachments (RDs), combined rhegmatogenous and tractional RDs, or vitreomacular traction/ERMs. A review of patients who underwent surgery for the sequelae of PDR found that surgeons reported that iOCT provided valuable information in 50.6% of cases and altered surgical decision making in 26% of cases.23 iOCT may be useful, especially in eyes with vitreous hemorrhage that could not be assessed with OCT preoperatively.23,24 Moreover, in tractional RD cases it can be used during membrane peeling and assessment of surgical dissection planes. Other reported uses include visualization of cannula placement during viscodissection and in identifying peripheral or macular holes/breaks, guiding choice for tamponade agent.23
SCENARIO NO. 4: RHEGMATOGENOUS RD
In a post-hoc analysis of eyes undergoing RD repair in the DISCOVER study, iOCT was determined to provide valuable information to surgeons in 36% of cases.25 Examples of helpful feedback included conformation of a posterior vitreous detachment, identification of residual subretinal fluid after PFO placement, confirmation of retinal reattachment, identification of the need for retinectomy, visualization of an occult MH, identification of a preretinal membrane, and identification of a retinal cyst (Figure 3).25 The utility of feedback gained from iOCT was felt to be higher in complex RD repairs than with primary, noncomplex repairs (50% versus 22%, P < .05).25 More investigation is needed to assess the outcomes of RD repair surgery with and without using iOCT.
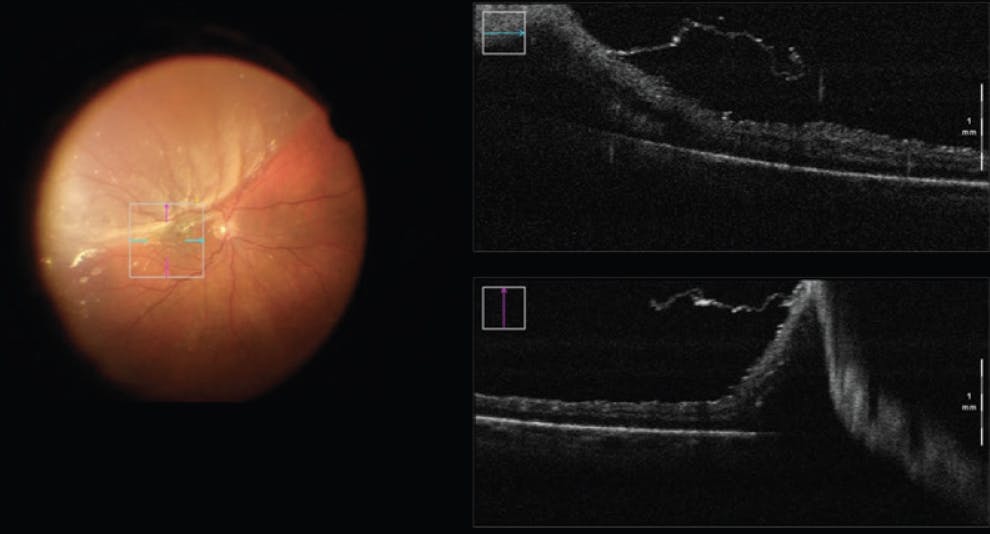
Figure 3. iOCT helped to identify an ERM during RD repair, which indicated the need for a membrane peel.
Image courtesy of Aleksandra V. Rachitskaya, MD. FASRS
SCENARIO NO. 5: UVEITIS
In cases where an infiltrative condition such as malignancy, amyloidosis, or atypical infection is suspected, a chorioretinal biopsy may be warranted to obtain a definitive diagnosis.26 iOCT can be useful in determining the site to biopsy and establishing if there is enough volume of subretinal material to allow for a successful biopsy.26 In the DISCOVER study, iOCT affected the surgical procedure in five of seven eyes undergoing chorioretinal biopsy, mostly in helping to plan the biopsy location based on lesion size and site and for positioning the soft tip at the biopsy site.27
iOCT has been described as useful during the placement or replacement of the fluocinolone acetonide implant (Retisert, Bausch + Lomb), particularly for ensuring scleral wound integrity and closure at the implant site.27 This can be critical when operating on eyes that have undergone multiple prior procedures, resulting in scleral thinning.27
MORE TO DO
iOCT can provide real-time feedback during vitreoretinal surgery and can assist with surgical decision making. More investigation is needed to determine the tool’s ability to improve patient outcomes in prospective, randomized clinical trials.
1. Huang D, Swanson EA, Lin CP, et al. Optical coherence tomography. Science. 1991;254(5035):1178-1181.
2. Pujari A, Agarwal D, Chawla R, Kumar A, Sharma N. Intraoperative optical coherence tomography guided ocular surgeries: critical analysis of clinical role and future perspectives. Clin Ophthalmol. 2020;14:2427-2440.
3. Ehlers JP, Modi YS, Pecen PE, et al. The DISCOVER study 3-year results: feasibility and usefulness of microscope-integrated intraoperative oct during ophthalmic surgery. Ophthalmology. 2018;125(7):1014-1027.
4. Ehlers JP, Dupps WJ, Kaiser PK, et al. The prospective intraoperative and perioperative ophthalmic imaging with optical coherence tomography (PIONEER) study: 2-year results. Am J Ophthalmol. 2014;158(5):999-1007.
5. Yee P, Sevgi DD, Abraham J, et al. IOCT-assisted macular hole surgery: outcomes and utility from the DISCOVER study. British J Ophthalmol. 2021;105(3):403-409.
6. Jaycock PD, Bunce C, Xing W, et al. Outcomes of macular hole surgery: implications for surgical management and clinical governance. Eye. 2005;19(8):879-884.
7. Bae K, Kang SW, Kim JH, Kim SJ, Kim JM, Yoon JM. Extent of internal limiting membrane peeling and its impact on macular hole surgery outcomes: a randomized trial. Am J Ophthalmol. 2016;169(2013):179-188.
8. Tao J, Chen H, Zhu L, et al. Macular hole edge morphology predicts restoration of postoperative retinal microstructure and functional outcome. BMC Ophthalmol. 2020;20(1):1-7.
9. Ehlers JP, Uchida A, Srivastava SK, Hu M. Predictive model for macular hole closure speed: Insights from intraoperative optical coherence tomography. Transl Vis Sci Technol. 2019;8(1):18.
10. Ehlers JP, Khan M, Petkovsek D, et al. Outcomes of intraoperative OCT–assisted epiretinal membrane surgery from the PIONEER study. Ophthalmol Retina. 2018;2(4):263-267.
11. Lorusso M, Micelli Ferrari L, Gisotti EN, et al. Success of iOCT in surgical management of ERM peeling. Eur J Ophthalmol. 2022;32(5):3116-3120.
12. Rodrigues EB, Meyer CH, Mennel S, Farah ME. Mechanisms of intravitreal toxicity of indocyanine green dye: implications for chromovitrectomy. Retina. 2007;27(7):958-970.
13. Sakamoto T, Itaya K, Noda Y, Ishibashi T. Retinal pigment epithelial changes after indocyanine green-assisted vitrectomy. Retina. 2002;22(6):794-796.
14. Tuifua TS, Sood AB, Abraham JR, et al. Epiretinal membrane surgery using intraoperative OCT-guided membrane removal in the DISCOVER study versus conventional membrane removal. Ophthalmol Retina. 2021;5(12):1254-1262.
15. Ehlers JP, Tam T, Kaiser PK, Martin DF, Smith GM, Srivastava SK. Utility of intraoperative optical coherence tomography during vitrectomy surgery for vitreomacular traction syndrome. Retina. 2014;34(7):1341-1346.
16. Bruyère E, Philippakis E, Dupas B, Nguyen-Kim P, Tadayoni R, Couturier A. Benefit of intraoperative optical coherence tomography for vitreomacular surgery in highly myopic eyes. Retina. 2018;38(10):2035-2044.
17. Itoh Y, Inoue M, Kato Y, Koto T, Hirakata A. Alterations of foveal architecture during vitrectomy for myopic retinoschisis identified by intraoperative optical coherence tomography. Ophthalmologica. 2019;242(2):87-97.
18. Gregori NZ, Lam BL, Davis JL. Intraoperative use of microscope-integrated optical coherence tomography for subretinal gene therapy delivery. Retina. 2019;39:S9-S12.
19. Vasconcelos HM, Lujan BJ, Pennesi ME, Yang P, Lauer AK. Intraoperative optical coherence tomographic findings in patients undergoing subretinal gene therapy surgery. Int J Retina Vitreous. 2020;6(1):1-10.
20. Hsu ST, Gabr H, Viehland C, et al. Volumetric measurement of subretinal blebs using microscope-integrated optical coherence tomography. Transl Vis Sci Technol. 2018;7(2):19.
21. Smith AG, Cost BM, Ehlers JP. Intraoperative OCT-assisted subretinal perfluorocarbon liquid removal in the DISCOVER study. Ophthalmic Surg Lasers Imaging Retina. 2015;46(9):964-966.
22. Ehlers JP, Petkovsek DS, Yuan A, Singh RP, Srivastava SK. Intrasurgical assessment of subretinal tPA injection for submacular hemorrhage in the PIONEER study utilizing intraoperative OCT. Ophthalmic Surg Lasers Imaging Retina. 2015;46(3):327-332.
23. Khan M, Srivastava SK, Reese JL, Shwani Z, Ehlers JP. Intraoperative OCT-assisted surgery for proliferative diabetic retinopathy in the DISCOVER study. Ophthalmol Retina. 2018;2(5):411-417.
24. Tao J, Wu H, Chen Y, et al. Use of iOCT in vitreoretinal surgery for dense vitreous hemorrhage in a chinese population. Curr Eye Res. 2019;44(2):219-224.
25. Abraham JR, Srivastava SK, K Le T, et al. Intraoperative OCT-assisted retinal detachment repair in the DISCOVER study: impact and outcomes. Ophthalmol Retina. 2020;4(4):378-383.
26. Browne AW, Ehlers JP, Sharma S, Srivastava SK. Intraoperative optical coherence tomography-assisted chorioretinal biopsy in the DISCOVER study. Retina. 2017;37(11):2183-2187.
27. Kumar JB, Ehlers JP, Sharma S, Srivastava SK. Intraoperative OCT for uveitis-related vitreoretinal surgery in the DISCOVER study. Ophthalmol Retina. 2018;2(10):1041-1049.



-1_1674489004.jpg?auto=compress,format&w=70)


_1674488812.jpg?auto=compress,format&w=70)
_1784132761.jpg?auto=compress,format&w=75)











