

AT A GLANCE
- Up to half of optic disc pit cases can be complicated by optic pit-associated maculopathy.
- A wide variety of treatment strategies have been described for optic disc pit maculopathy, including laser photocoagulation at the temporal disc margin, intravitreal gas injection, macular buckling, and pars plana vitrectomy.
- Most published reports of various techniques for the management of optic disc pit-associated maculopathy involve a small number of cases with limited long-term follow-up.
Optic disc pit is a rare, congenital excavation of the optic nerve head. Its etiology is thought to be an incomplete closure of the embryonic fissure during fetal development, similar to other congenital optic disc anomalies such as morning glory syndrome and optic nerve colobomas.1 Optic pits are usually unilateral, although up to 15% are bilateral. Most pits are located at the inferotemporal aspect of the disc and appear as a grayish, oval-shaped depression on a fundoscopic examination (Figure).
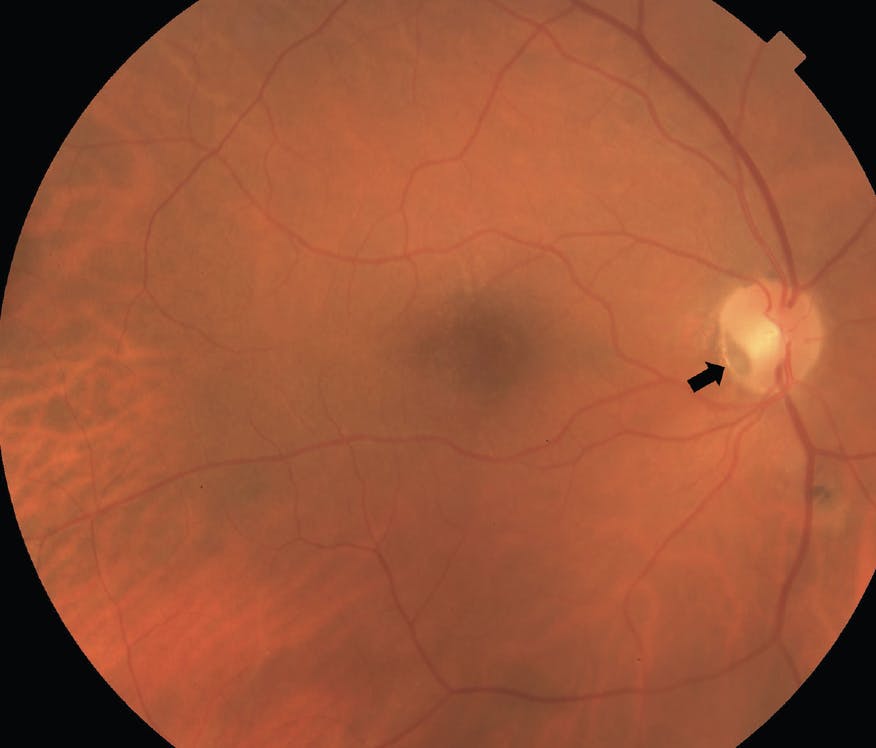
Figure. This fundus photograph demonstrates an optic disc pit in the inferotemporal margin of the optic nerve (arrow). There is no associated serous macular detachment in this case.
Although patients with optic disc pits are often asymptomatic, visual field defects have been described. The defects are most commonly an enlarged blind spot or a paracentral scotoma.1,2 However, up to half of the cases can be complicated by optic pit-associated maculopathy—retinoschisis-like changes and serous macular detachment—that can be associated with significant deterioration in vision.3 Optic pit maculopathy occurs equally in males and females and usually appears in the third or fourth decade of life.
CURRENT HYPOTHESES
The exact etiology of optic disc pit leading to serous retinal detachment remains unclear, although there are two leading hypotheses. The first postulates that vitreous traction on the optic disc pit and macula results in a negative pressure gradient, allowing vitreous fluid to enter through the pit and into the submacular space.1,4 In one series, vitreous traction was observed with OCT in the majority of patients with optic disc pit maculopathy.5 The second hypothesis suggests that the optic pit defect creates a direct communication between the subarachnoid and subretinal spaces, allowing cerebral spinal fluid (CSF) to create the serous retinal detachment.6 In support of this hypothesis, Kuhn et al presented a case report of a patient with optic disc pit associated serous detachment who underwent pars plana vitrectomy (PPV) with silicone oil.7 During an evaluation for persistent headaches years later, emulsified silicone oil was seen intracranially on MRI of the head. The emulsified oil presumably passed from the vitreous cavity through the optic disc pit into the CSF space then intracranially.
Although spontaneous resolution with improvement in symptoms has been reported, untreated optic disc pit maculopathy typically leads to progressive vision loss with overall poor outcomes.8-10 Therefore, specialists should offer treatment with minimal delay.
POTENTIAL TREATMENTS
Because optic disc pit maculopathy is rare, there is no clear consensus on the most effective treatment. A wide variety of treatment strategies have been described, including laser photocoagulation at the temporal disc margin, intravitreal gas injection, macular buckling, and PPV.
The rationale for laser photocoagulation at the temporal disc margin is that the chorioretinal adhesion created by the laser will serve as a barrier between the optic disc pit and the subretinal space. In practice, the time for improvement is often long, and the laser location over the maculopapular bundle can cause significant visual field defects.11 As a result, this treatment modality—when performed in isolation—has largely fallen out of favor.
The reasoning behind intravitreal gas injection is that pneumatic displacement may induce a posterior vitreous detachment while sealing the optic pit, resulting in macular reattachment. This technique was used in several small series with an overall 50% success rate for macular reattachment. However, more than one injection was often necessary.12
With macular buckling surgery, complete resorption of fluid has been reported in as high as 85% of cases. Furthermore, improvement in visual acuity has been demonstrated over long-term follow-up with low rates of recurrences.13,14 While impressive, these results have not been replicated, and this technique has not been widely adopted.
PPV is often the treatment of choice, either alone or in combination with gas tamponade, laser photocoagulation, and internal limiting membrane (ILM) peeling. Induction of a complete posterior vitreous detachment to remove vitreous traction on the optic pit is thought to be critical for macular reattachment. Gas tamponade in combination with PPV has been suggested to help seal the optic pit and move the subretinal fluid away from the macula.15 Endolaser on the temporal aspect of the optic nerve at the time of PPV carries the same risk of visual field defect and vision loss as when performed alone.16 ILM peeling can help to eliminate tangential traction, and multiple reports have described good visual outcomes with PPV with ILM peeling.17 However, some authors have reported good results without ILM peeling, and they believe it to be unnecessary.16
Other techniques include directly covering or plugging the optic disc pit with an ILM flap, autologous scleral flap, human amniotic membrane, or fibrin glue. A few cases using an inverted ILM flap to cover the optic disc pit in conjunction with gas tamponade have been reported with improvement in both vision and anatomy.18-20 However, in cases where the ILM was peeled in the foveal area to create a large ILM flap, postoperative macular holes can develop with a resulting drop in vision.21 Therefore, in cases with a thin retina over the fovea—similar to cases with high myopia—a foveal-sparing ILM peel should be considered.
Some authors advocate for plugging the pit with ILM, with the argument that covering the optic disc pit may prevent vitreous fluid from entering the subretinal space via the pit but doesn’t prevent CSF from entering the subretinal space. Plugging the pit may prevent both potential sources of fluid from entering the subretinal space. One case series comparing a simple ILM flap versus plugging the optic pit with ILM demonstrated faster resolution of fluid with the plugging technique.22
The use of an autologous scleral tissue flap to cover or plug the optic disc pit has been reported. A few small case series showed resolution of fluid with improvement in vision.15,23,24 One comparative case series showed similar outcomes between eyes that had an ILM flap versus those that had an autologous scleral tissue flap.24 Autologous fibrin prepared from the patient’s whole blood has also been used.25 A report of two cases that previously did not improve with PPV and ILM peeling subsequently underwent PPV with autologous fibrin injected over the pit to seal it. Anatomic improvement was noted in both cases with the resolution of macular detachment. The use of fibrin glue over the optic pit has also been suggested.26 More recently, human amniotic membrane has been used in a case series of 11 patients to plug the optic disc pit and demonstrated excellent visual and anatomic outcomes at 12 months.27
Ooto et al used PPV with inner retinal fenestration using a bent 25-gauge needle in 18 patients without laser photocoagulation to achieve anatomic and functional improvement.28 This indicates that inner retinal fenestration can redirect fluid into the vitreous cavity instead of the retina.
TIME TO THINK LONG-TERM
Thus far, most published reports of various techniques in the management of optic disc maculopathy involve a small number of cases with limited long-term follow-up, and potential long-term complications such as visual field loss may not yet be present. Furthermore, most studies did not perform formal visual field evaluation. The risk of direct mechanical injury to the optic nerve is likely highest with techniques where additional material is implanted directly into the optic nerve pit. These cases are challenging to manage, and there are no established guidelines for treatment. Currently, the predominant treatment is PPV with different adjuvant therapies. There are limited studies comparing different surgical approaches, and additional studies are needed to provide clarity on the optimal surgical approach.
1. Brown GC, Shields JA, Goldberg RE. Congenital pits of the optic nerve head. II. Clinical studies in humans. Ophthalmology. 1980;87(1):51-65.
2. Shah SD, Yee KK, Fortun JA, Albini T. Optic disc pit maculopathy: a review and update on imaging and treatment. Int Ophthalmol Clin. 2014;54(2):61-78.
3. Bonnet M. Serous macular detachment associated with optic nerve pits. Graefes Arch Clin Exp Ophthalmol. 1991;229(6):526-532.
4. Georgalas I, Ladas I, Georgopoulos G, Petrou P. Optic disc pit: a review. Graefes Arch Clin Exp Ophthalmol. 2011;249(8):1113-1122.
5. Theodossiadis PG, Grigoropoulos VG, Emfietzoglou J, Theodossiadis GP. Vitreous findings in optic disc pit maculopathy based on optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2007;245(9):1311-1318.
6. Ohno-Matsui K, Hirakata A, Inoue M, et al. Evaluation of congenital optic disc pits and optic disc colobomas by swept-source optical coherence tomography. Invest Ophthalmol Vis Sci. 2013;54:7769-7778.
7. Kuhn F, Kover F, Szabo I, Mester V. Intracranial migration of silicone oil from an eye with optic pit. Graefes Arch Clin Exp Ophthalmol. 2006;244(10):1360-1362.
8. Patton N, Aslam SA, Aylward GW. Visual improvement after long-standing central serous macular detachment associated with an optic disc pit. Graefes Arch Clin Exp Ophthalmol. 2008;246(8):1083-1085.
9. Vedantham V, Ramasamy K. Spontaneous improvement of serous maculopathy associated with congenital optic disc pit: an OCT study. Eye (Lond). 2005;19(5):596-599.
10. Sobol WM, Blodi CF, Folk JC, Weingeist TA. Long-term visual outcome in patients with optic nerve pit and serous retinal detachment of the macula. Ophthalmology. 1990;97(11):1539-1542.
11. Mustonen E, Varonen T. Congenital pit of the optic nerve head associated with serous detachment of the macula. Acta Ophthalmol (Copenh). 1972;50(5):689-698.
12. Akiyama H, Shimoda Y, Fukuchi M, et al. Intravitreal gas injection without vitrectomy for macular detachment associated with an optic disk pit. Retina. 2014;34(2):222-227.
13. Theodossiadis GP, Theodossiadis PG. The macular buckling technique in the treatment of optic disk pit maculopathy. Semin Ophthalmol. 2000;15(2):108-115.
14. Theodossiadis GP, Chatziralli IP, Theodossiadis PG. Macular buckling in optic disc pit maculopathy in association with the origin of macular elevation: 13-year mean postoperative results. Eur J Ophthalmol. 2015;25(3):241-248.
15. Travassos AS, Regadas I, Alfaiate M, et al. Optic pit: novel surgical management of complicated cases. Retina. 2013;33(8):1708-1714.
16. Avci R, Yilmaz S, Inan UU, et al. Long-term outcomes of pars plana vitrectomy without internal limiting membrane peeling for optic disc pit maculopathy. Eye (Lond). 2013;27(12):1359-1367.
17. Rizzo S, Belting C, Genovesi-Ebert F, et al. Optic disc pit maculopathy: the value of small-gauge vitrectomy, peeling, laser treatment, and gas tamponade. Eur J Ophthalmol. 2012;22(4):620-625.
18. Mohammed OA, Pai A. Inverted autologous internal limiting membrane for management of optic disc pit with macular detachment. Middle East Afr J Ophthalmol. 2013;20(4):357-359.
19. Hara R, Tsukahara Y, Simoyama T, Mori S. Refined internal limiting membrane inverted flap technique for intractable macular detachment with optic disc pit. Case Rep Ophthalmol. 2017;8(1):208-213.
20. Sborgia G, Recchimurzo N, Sborgia L, et al. Inverted internal limiting membrane-flap technique for optic disk pit maculopathy: morphologic and functional analysis. Retin Cases Brief Rep. 2021;15(1):31-37.
21. Shukla D, Kalliath J, Tandon M, Vijayakumar B. Vitrectomy for optic disk pit with macular schisis and outer retinal dehiscence. Retina. 2012;32(7):1337-1342.
22. Ravani R, Kumar A, Karthikeya R, et al. Comparison of inverted ILM-stuffing technique and ILM peeling alone for optic disc pit-associated maculopathy: long-term results. Ophthalmic Surg Lasers Imaging Retina. 2018;49(12):e226–e232.
23. Shah PK, Karandikar SS, Narendran V. Scleral autograft for optic nerve head pit associated chronic maculopathy. Ophthalmic Surg Lasers Imaging Retina. 2017;48(3):251-254.
24. Babu N, Kohli P, Ramasamy K. Comparison of various surgical techniques for optic disc pit maculopathy: vitrectomy with internal limiting membrane (ILM) peeling alone versus inverted ILM flap “plug” versus autologous scleral “plug.” Br J Ophthalmol. 2020;104(11):1567-1573.
25. Ozdek S, Ozdemir HB. A new technique with autologous fibrin for the treatment of persistent optic pit maculopathy. Retina Cases Brief Rep. 2017;11(1):75-78.
26. Almeida DRP, Chin EK, Arjmand P, et al. Fibrin glue and internal limiting membrane abrasion for optic disc pit maculopathy. Ophthalmic Surg Lasers Imaging Retina. 2018;49(12):e271–e277.
27. Caporossi T, D’Amico G, Tartaro R, et al. Optic disk pit maculopathy treatment using a human amniotic membrane patch: one-year results. Am J Ophthalmol. 2022;240:30-36.
28. Ooto S, Mittra RA, Ridley ME, et al. Vitrectomy with inner retinal fenestration for optic disc pit maculopathy. Ophthalmology. 2014;121(9):1727-1733.





_1674488812.jpg?auto=compress,format&w=70)
-1_1674489004.jpg?auto=compress,format&w=70)
_1784132761.jpg?auto=compress,format&w=75)











