



The 13th annual Vit-Buckle Society meeting, held March 20 – 22, 2025, in Austin, Texas, was another feat of clinical and surgical education, professional growth, and networking. With a wild west theme, speakers and attendees swaggered on stage to discuss challenging surgical cases, hurdles to patient care, wellness, and more.
A highlight of the meeting was a unique panel discussion that focused on complex bilateral retinal detachment (RD) cases. Moderators Tavish Nanda, MD, and Carl D. Regillo, MD, introduced several cases that mirrored real-life challenges, including patients walking in late on a Friday afternoon with retinal pathology in both eyes simultaneously. The goal of the panel was to explore each panelist’s clinical reasoning and the variation in surgical approaches among experts across different practice settings. Each case included a survey of the audience to compare general consensus against the panelists. Here is what María H. Berrocal, MD; Steve Charles, MD; Peter J. Kertes, MD; and Ashleigh L. Levison, MD, had to say (Figure 1).

Figure 1. During the surgical scenarios panel (from left to right), Drs. Nanda, Charles, Kertes, Berrocal, Levison (inset left), and Regillo (inset right) discussed their various approaches to the surgical management of bilateral RDs. Images courtesy of Kevin Caldwell Photography.
CASE NO. 1: GIANT RETINAL TEAR
A 60-year-old phakic woman presented with a 1-week shadow in her left eye. Her VA was 20/30 OU. Dilated fundus examination reveal a nasal detachment with a giant retinal tear (GRT) in the left eye and an unexpected superotemporal RD in the right eye with multiple breaks (Figure 2). Each eye was still macula-on.
The audience was asked which eye should be treated first. The majority selected the left eye due to the presence of a GRT, although 14% supported simultaneous bilateral repair. Dr. Berrocal recommended treating the left eye first with a vitrectomy, scleral buckle, and silicone oil. She preferred to wait to perform a straight buckle (sponge, no drainage) on the right eye until 2 days later. Dr. Regillo rarely performs bilateral surgery but supported operating 1 to 2 weeks apart.
Dr. Charles opposed buckling altogether, calling himself “Mr. Anti-Buckle” and highlighting the possible buckle-related complications of refractive error, diplopia, discomfort, and longer operating time. He advocated for vitrectomy with silicone oil in the left eye and emphasized the importance of removing the oil within a month to avoid complications such as macular edema or emulsification. On the other end of the spectrum, Dr. Kertes suggested a pneumatic retinopexy in both eyes on the same day, despite the level of pathology. He emphasized his high success rates, even with GRTs, and saw no need to delay treatment.
The Surgical Plan
After the discussion Dr. Nanda revealed the surgeon’s actual management, which involved a vitrectomy with silicone oil and an encircling buckle for the GRT within 24 hours. The surgeon chose close follow-up to allow the left eye to recover before surgery on the right. By 1 week, however, the right eye was now 20/150 with foveal encroachment. The surgeon chose a vitrectomy with gas and an encircling buckle. The surgeon chose a buckle due to the patient’s atypical presentation, possibility of an underlying vitreopathy, and lens status. Dr. Berrocal noted that pinhole glasses can sometimes be helpful in these bilateral cases to slow progression of an RD as an alternative to bilateral patching. Six months after oil removal and cataract surgery, the patient’s VA was 20/40 OU.

Figure 2. The VBS panel first discussed this patient, who presented with a focal superior detachment in the right eye and a GRT in the left eye. Images courtesy of Tavish Nanda, MD.
CASE NO. 2: FOCAL AND MACULA-OFF
In the second case, the patient was pseudophakic with a small superonasal RD in the right eye and a more extensive superotemporal RD in the left eye (Figure 3). The right eye had no clear visible break, likely due to a limited view around the edge of the IOL. The left eye was macula-off with multiple breaks, both nasally and superotemporally.
The audience largely agreed on prioritizing the left eye. Dr. Charles recommended laser demarcation for the small, localized RD in the right eye and a vitrectomy with “medium-term” PFO in the left eye. He shared that he has used PFO in more than 1,300 cases in 23 years of practice and that it’s particularly useful for inferior detachments. The benefit, he noted, is that patients can function normally for 2 weeks before staged PFO removal, with less discomfort and no induced refractive error. If the breaks are more superior (eg, 10 to 2 clock hours), he uses gas.
In terms of surgical timing, Dr. Berrocal said she typically operates within 1 week of macula-off symptoms. Dr. Levison prefers to get the patient to the OR within 3 days, if possible.
For the right eye, Dr. Kertes stated that if there is no visual field defect and the detachment is anterior to the equator, laser barricade is appropriate. Dr. Charles agreed, adding that only two to three confluent rows are typically needed for a sufficient barricade to prevent an iatrogenic scotoma. Although a pneumatic can be considered, especially with a superior RD, the panel generally agreed that laser break-through is rare.
The majority of the audience chose a vitrectomy with gas for the left eye. For the right eye, the audience agreed with laser demarcation.
The Surgical Plan
Surgical management in this case included in-office laser for the right eye and a vitrectomy with endolaser and 15% C3F8 gas for the left eye. The panelists also discussed the long-term follow-up strategy for patients with RDs. Dr. Kertes rarely follows uncomplicated RD repairs more than 2 months. In contrast, Dr. Charles explained that visual improvement can continue up to 18 months post-surgery. From the audience, Yoshihiro Yonekawa, MD, shared data from his team’s review of thousands of RD cases at Wills Eye Hospital in Philadelphia, noting that 1.4% of cases can redetach even after 1 year, more commonly after pneumatic retinopexies.
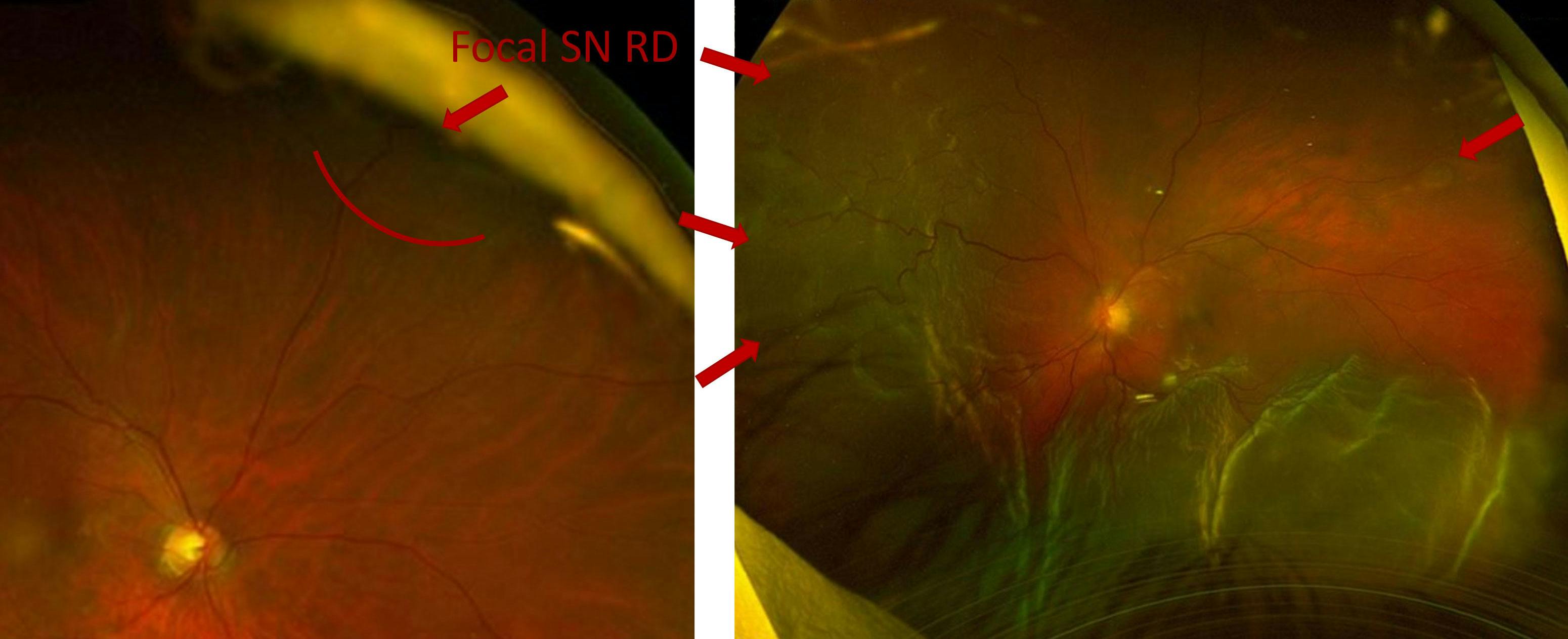
Figure 3. This pseudophakic patient presented with a small superonasal RD in the right eye and a superotemporal macula-off RD in the left eye with multiple breaks. Images courtesy of Tavish Nanda, MD.
CASE NO. 3: PEDIATRIC RD
The third case involved a 15-year-old female patient who presented with a mild shadow in her vision. Examination noted bilateral, macula-on, inferonasal RDs, with multiple large retinal breaks (Figure 4). There was no posterior vitreous detachment (PVD) in either eye. There was no notable family history or ocular trauma.
Dr. Berrocal recommended a staged approach with encircling scleral buckles in each eye. In a young patient with no PVD and atypical detachments, she saw the encircling buckle as the safest, most reliable approach. Timing between surgeries should be 2 to 3 days, she said, as opposed to simultaneous bilateral interventions in a young patient.
Dr. Kertes, on the other hand, proposed pneumatic retinopexy for each eye. He shared that the youngest pneumatic patient he has treated was 9 years old. Even with multiple inferonasal breaks, pneumatic retinopexy was effective, he said, and the lack of induced myopia or need for surgery made it preferable for the patient and their family.
The audience was in general agreement, with most recommending a primary buckle for both eyes.
The Surgical Plan
In this case, the surgeon proceeded with a scleral buckle and cryotherapy in the left eye within 1 week due to a greater “shadow” and larger breaks. One month later, a similar procedure with a scleral buckle and cryotherapy was performed in the right eye. There was no discernible progression over that timeframe.
In young patients without PVD, especially with inferior cases, some delay can be acceptable as long as symptoms are stable, the panelists agreed. However, Dr. Regillo cautioned that, in cases of Stickler syndrome or other heritable vitreoretinopathies, RDs may progress more rapidly. He advised considering genetic testing. The panelists also addressed the use of pneumatic retinopexy in young patients, acknowledging that gas can hasten PVD formation, increasing the risk of new breaks. They agreed that such cases require close follow-up when a pneumatic is performed.

Figure 4. The final case discussed during the panel involved a 15-year-old patient who presented with bilateral inferonasal RDs and no PVD in either eye. Images courtesy of Tavish Nanda, MD.
WHAT’S YOUR BILATERAL RD APPROACH?
This session highlighted the spectrum of expert approaches to complex bilateral RD cases. While surgical philosophy varied, several consistent themes emerged. Scleral buckles remain polarizing; Drs. Berrocal and Regillo use them often, especially in young patients or those with inferior pathology, while Dr. Charles avoids them altogether. Pneumatic retinopexy received strong advocacy from Dr. Kertes, who argued for its broader use even in complex and bilateral settings. Dr. Charles supports the routine use of PFO as a valuable option for inferior detachments, particularly for functional preservation. Laser barricade remains a safe, effective strategy for small RDs, especially if they are anterior and without symptomatic field loss.
Long-term follow-up strategies varied based on practice models, but the consensus was that most redetachments happen within 2 months and that patients should be educated on that risk. Overall, the panel emphasized individualized care, early intervention, and patient-centered decision making as the cornerstones of success in managing bilateral RDs.
SAVE THE DATE: April 9 – 11, 2026
14th Annual Vit-Buckle Society Meeting
Las Vegas




-1_1748961738.jpg?auto=compress,format&w=70)







_1784132761.jpg?auto=compress,format&w=75)











